How PTSD Is Treated: From First-Line Care to Advanced Options

Post-traumatic stress disorder (PTSD) isn’t a “weakness” or a character flaw. It’s a mental health condition where your nervous system gets stuck on high alert. It develops when the brain and body stay in survival mode long after a life-threatening situation—something you experienced or witnessed—has passed. While PTSD can be debilitating, the good news is that effective treatments exist. But PTSD treatment isn’t one-size-fits-all—and knowing what actually works, what doesn’t, and when to switch gears can change everything.
Finding the right PTSD treatment can feel like a maze—especially when you’re already exhausted from carrying the aftermath of something that never should have happened. If you’ve been diagnosed with PTSD (or strongly suspect you have it), you may be staring down a flood of options—therapy, medication, newer brain-based treatments—and wondering what actually works, what’s hype, and what comes next if your first attempt didn’t help.
I know what it’s like to feel shaken after trauma. Birth trauma and a scary hospital stay left me struggling to feel safe in my own body again. Even three years later, my body remembers: the sick, queasy drop in my stomach when I walk into a medical building, the jolt of dread when I hear the beep of a blood pressure monitor. That’s the thing about trauma—it doesn’t just live in memory. It shows up in the body, in reactions you didn’t choose, and in ways that can quietly (or loudly) interfere with daily life.
For some people, that ongoing survival response develops into post-traumatic stress disorder—a condition where the mind and body keep reliving the past as if the danger is still present. But PTSD is treatable, and what’s more, treatment isn’t one-size-fits-all—it’s a series of personalized steps. Whether you’re exploring therapy for PTSD for the first time, feeling stuck after trying something that didn’t work, or looking for more advanced trauma treatment, there are many paths forward.
In this article, we’ll break down what evidence-based PTSD help actually looks like—what first-line treatments are, when and how options can be combined, what to consider if standard approaches haven’t worked, and how to advocate for care that fits you. No vague reassurance. Just clear, practical guidance to help you make sense of your options and move toward healing from PTSD, at your pace and on your terms.
How is PTSD treated?
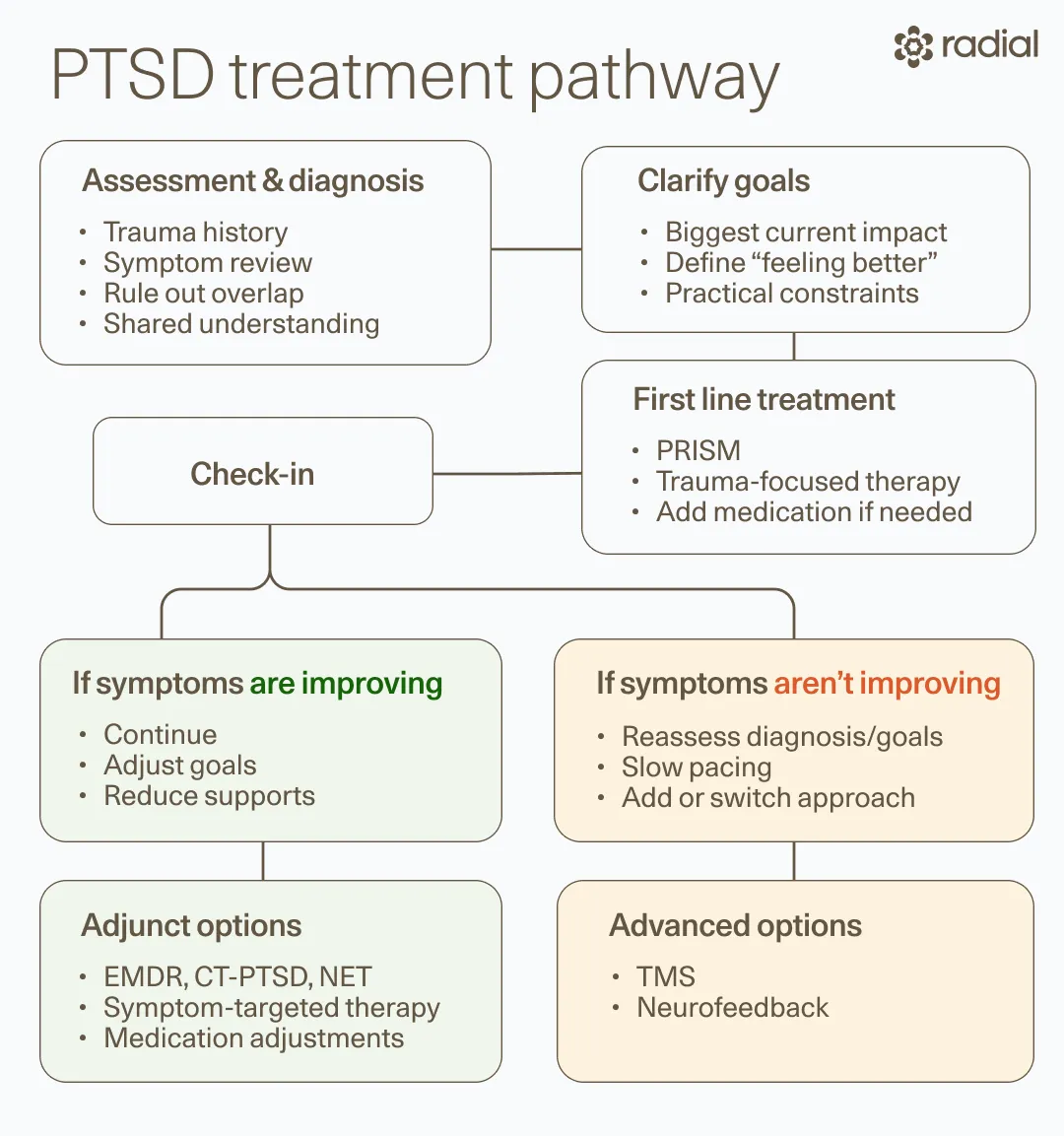
Before we dive into how PTSD is treated, everything starts with getting the diagnosis right. “PTSD is often misdiagnosed,” says Ahmed Tahseen, MD, clinical advisor at Radial, medical director at Biohaven Therapeutics, and clinical instructor of psychiatry at Yale University. That’s because its symptoms overlap with many other conditions, including depression, bipolar disorder, anxiety disorders, and even ADHD, Dr. Tahseen says. Without a clear diagnosis, treatment can miss the mark.
Making a proper PTSD diagnosis is even more challenging because trauma isn’t always caused by one big, overwhelming event. Research now shows trauma can also develop after repeated or less obvious stressors. “Many different types of difficult experiences can build up and cause PTSD,” says Dr. Tahseen—things like abusive relationships, bullying, racism, sexism, or growing up in violent environments. That’s why a thorough history, often starting in childhood, is critical for accurate diagnosis, he adds.
As a result, PTSD also doesn’t look the same in everyone, and it doesn’t always look like the movies, says Dr. Tahseen. Case in point: Not everyone has vivid flashbacks. PTSD can show up across several domains: re-experiencing, avoidance, negative changes in mood and thinking, and heightened arousal or reactivity. These symptoms can affect nearly every area of life—sleep, appetite, work, relationships, and the ability to feel present or safe, he says.
This variability is exactly why treatment must be tailored. “PTSD shows up in such personalized, vastly different ways,” says Dr. Tahseen, “which is why treatment plans are equally individualized.” A good plan starts by identifying which symptoms are most disruptive and where life feels most constrained.
Sometimes, the first step is simply accepting the diagnosis. For some people, hearing “PTSD” is hard. It’s not always easy to accept that something undeserved or painful happened, says Dr. Tahseen. Many of us survive by minimizing or pushing through, and naming trauma can feel destabilizing. In those cases, “understanding the diagnosis [itself] can be a part of the treatment and should be approached with care and the right pacing,” he explains.
Next comes goal-setting because progress needs a target. Clear goals help guide treatment and measure whether it’s working, says Dr. Tahseen. These often focus on practical markers: showing up at work, feeling more connected in relationships, or improving sleep, mood, and appetite, he says. Tracking these changes over time helps everyone know if things are moving in the right direction.
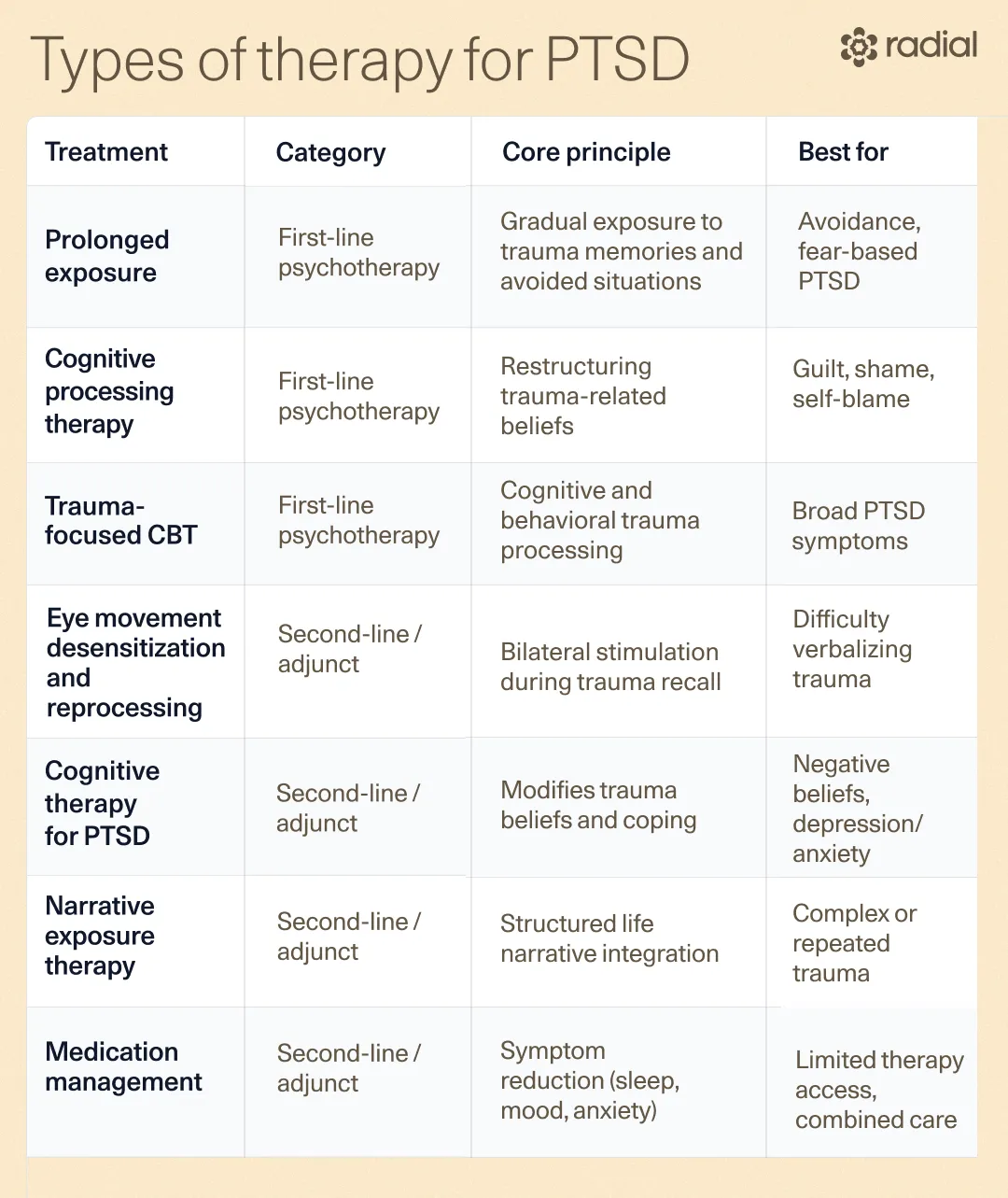
Choosing the appropriate therapy is also a huge part of an effective PTSD treatment plan. There are many options, but “the mainstay of PTSD treatments is psychotherapy,” says Dr. Tahseen. Per APA clinical guidelines, first-line treatments typically include cognitive behavioral therapy (CBT), cognitive processing therapy (CPT), and prolonged exposure therapy. “Some [of these] have reasonably good remission rates,” says Dr. Tahseen. For example, about half of the people who complete CPT no longer meet criteria for PTSD, he says.
That said, prolonged exposure and other exposure-based treatments aren’t always the first move. These evidence-based therapies involve revisiting or integrating traumatic memories, but “sometimes focusing on symptoms first can be very powerful,” says Dr. Tahseen. Insomnia, for example, which is common in PTSD, can worsen everything else. “CBT-I (cognitive behavioral therapy for insomnia) is highly effective,” says Dr. Tahseen, and in some cases, improving sleep alone can reduce PTSD symptoms.
Depending on symptoms and access to therapy, medication (considered a second-line treatment per the APA clinical guidelines) may be part of the plan as well. But in PTSD, meds are best thought of as symptom management rather than as a cure. “Medications generally have low effect sizes,” says Dr. Tahseen. And sadly, many people with PTSD end up cycling through medications that don’t meaningfully help, he explains.
Connect with our Clinicians


.webp)
Other options may come into play when needed. Additional second-line PTSD therapies like eye movement desensitization and reprocessing (EMDR) and newer treatments like neurofeedback and transcranial magnetic stimulation (TMS) can be valuable additions, depending on the person and their response to first-line care.
Real-world constraints matter, too. Time, cost, access, and emotional bandwidth all affect what’s realistic. A treatment plan only works if it’s feasible. There’s no benefit in designing a “perfect” plan that can’t be followed.
That’s why collaboration between you and your provider is super important at this planning stage. At the core, effective care relies on shared decision-making. Providers should clearly explain options, risks, and expected outcomes and work with patients to tailor goals and approaches based on preferences, needs, and capacity.
To sum it up: PTSD treatment isn’t one-size-fits-all; it’s an incremental, individualized process. If one approach doesn’t work, that’s not a failure—it’s information. With the right tools and support, healing is absolutely possible.
A quick note on clinical guidelines
Multiple countries have developed evidence-based guidelines for PTSD treatment, and recommendations may vary slightly. For this article, we reference the American Psychological Association (APA) guidelines. Other widely used frameworks include:
- ISTSS Treatment Guidelines
- Australian Guidelines for Acute Stress Disorder and PTSD
- NICE PTSD Guidelines (UK)
- U.S. VA/DoD Clinical Practice Guidelines
- American Psychiatric Association Practice Guidelines
All reinforce the same core message: PTSD is treatable, and care works best when it’s individualized, evidence-based, and collaborative.
First-line PTSD treatments
First-line PTSD treatments are backed by decades of research and are usually the first place clinicians turn when building a treatment plan. Here are the first-line PTSD treatments, according to the APA clinical guidelines.
Cognitive behavioral therapy (CBT)
Cognitive behavioral therapy (CBT) is about learning to spot thought and behavior loops that keep trauma stuck on repeat, then gently replacing them with more balanced patterns. For PTSD, CBT helps you understand how trauma shaped your beliefs, reactions, and avoidance, and gives you tools to take some of that power back.
Two CBT approaches with the strongest track records:
- Cognitive Processing Therapy (CPT): focuses on unpacking the beliefs you formed around your trauma and reframing them in ways that are more accurate.
- Prolonged Exposure Therapy: with careful guidance, you gradually face memories or situations you’ve been avoiding, teaching your brain that the danger has passed and you’re safe now.
CBT is one of the most well-studied, evidence-backed treatments for PTSD across ages and trauma types, but it’s not a magic bullet. Research shows that up to half of people may not respond fully, often due to co-occurring mental health conditions or the nature of the trauma itself. And because exposure-based work can be emotionally intense, some people find it hard to stick with. Bottom line: CBT can be life-changing for many, but not all, and that’s okay.
What happens if first-line treatment isn’t working?
This is common. One meta-analysis found the average nonresponse rate to first-line psychological treatments for PTSD was 39.23%. And it doesn’t mean you’re doing anything wrong.
In fact, even determining whether a treatment is doing its job can be tricky. Honestly, “this is a difficult question,” says Dr. Tahseen. Some PTSD treatments, like cognitive processing therapy (CPT), follow a fairly set timeline—typically 12 sessions over about three months—making it easier to check progress, he says. But many others, including EMDR, IFS, and exposure-based therapies, don’t come with a built-in clock. There’s no universal deadline for deciding whether they’re “working.”
So how do you tell if a treatment is the right fit? According to Dr. Tahseen, it’s not a pass/fail test—it’s a collaboration. Clinicians may use assessments or symptom scales (like the CAPS-5 or PCL-5) to track change. But just as important: how you feel. “I advise patients to listen to themselves,” he says. Sharing what’s improving, what’s stuck, and what feels off helps you and your clinician decide together whether to stay the course or pivot.
One of the clearest signs you’re on the right track is real-life progress. Are you functioning better at work? Sleeping more consistently? Feeling more emotionally regulated? Reconnecting in relationships? If the needle is moving in these areas—even gradually—that’s meaningful progress. “Ideally, you should know if you’re trending toward your goals in two to three months,” says Dr. Tahseen.
Second-line PTSD treatments
Per the APA’s clinical guidelines, these second-line PTSD treatments come into play when symptoms persist or a different approach is needed.
Cognitive therapy (CT-PTSD)
This therapy addresses the meaning your brain has attached to the trauma. Cognitive therapy for PTSD (CT-PTSD) focuses on identifying and changing the unhelpful interpretations you’ve developed about the trauma and its aftermath (things like distorted self-blame, a constant sense of danger, or memories that feel fragmented and stuck in the present).
The goal isn’t to erase the memory—it’s to stop it from running your life. Through treatment, you and your therapist work to reshape pessimistic beliefs and reorganize traumatic memories so they’re less intrusive. At the same time, you’ll tackle coping habits—like avoidance or mental replay—that may have helped you survive before, but are now keeping PTSD symptoms in place.
And yes, it actually works for a wide range of people. In one outpatient clinic study, CT-PTSD significantly improved PTSD symptoms, as well as reduced depression and anxiety, across patients with many different types of traumas.
Eye Movement Desensitization and Reprocessing (EMDR)
Eye movement desensitization and reprocessing (EMDR) is all about helping your brain reprocess traumatic memories so they don’t hit as hard. During sessions, you recall distressing events while following a rhythmic back-and-forth stimulus, like moving lights, taps, or sounds. The idea is that this bilateral stimulation helps the brain “re-file” painful memories, dialing down their emotional charge.
So what does the evidence say? Scientists still debate exactly how EMDR therapy works, but the results are hard to ignore. A solid body of research shows it can reduce PTSD symptoms, which is why the APA recommends it as a second-line treatment.
Another huge plus: EMDR translates well to telehealth, making it more accessible for people who prefer (or need) virtual care.
Narrative exposure therapy
Trauma has a way of shrinking your identity down to the worst things that happened to you. Narrative exposure therapy (NET) helps you zoom back out and reclaim the whole story.
Originally designed for people with repeated or long-term trauma (like refugees or survivors of chronic abuse), NET guides you in building a chronological “life story” where traumatic memories are woven into a broader narrative. This helps you process what happened, make meaning of it, and regain a sense of identity and control.
Usually delivered over 4–10 sessions, NET seems like a promising PTSD therapy, particularly in older adults. Meta-analyses suggest meaningful symptom improvement after treatment (and at follow-up), though researchers note that more high-quality studies are still needed.
Internal Family Systems
“My favorite psychotherapy is internal family systems for PTSD,” says Dr. Tahseen. Internal Family Systems (IFS) is a psychotherapy method that shows real promise in treating PTSD, but the science is still catching up.
In IFS, the mind is made up of different “parts” that developed around past experiences, especially trauma. Broadly, these fall into two categories: vulnerable parts that carry painful emotions, memories, or beliefs, and protective parts that step in to manage or avoid that pain (sometimes through behaviors that look like PTSD symptoms).
Rather than trying to eliminate symptoms, IFS focuses on building the capacity to approach vulnerable parts with mindfulness and self-compassion. Over time, this can help people tolerate, process, and integrate traumatic experiences more safely.
The early research is encouraging, but limited. One small pilot study suggests IFS may reduce PTSD symptoms, particularly in adults with childhood trauma, and one group-based, online proof of concept study showed promising symptom improvement. Still, larger, well-controlled trials are needed before stronger conclusions can be drawn.
IFS also “requires specialized training,” which means the pool of qualified therapists is still relatively small (though it is growing), says Dr. Tahseen.
Medications
Clinical guidelines don’t recommend medication alone or as the primary treatment, since only a handful have solid evidence behind them. Still, meds can be a helpful add-on in the right situations, especially when symptoms like anxiety, mood changes, or sleep disruption are getting in the way of healing. Here’s the quick, clear rundown of PTSD medications.
SSRIs
When it comes to meds used to treat PTSD, selective serotonin reuptake inhibitors (SSRIs) are the go-to. Two popular SSRIs—sertraline (Zoloft) and paroxetine (Paxil)—are FDA-approved specifically for PTSD.
SSRIs increase serotonin, a brain chemical involved in mood, sleep, and stress. According to clinical trials, SSRIs can help improve PTSD symptoms in some people, likely because higher serotonin levels may help with emotion regulation and reduce the intensity of negative emotions.
The trade-offs? Possible side effects like nausea, dizziness, sweating, headaches, sexual side effects, and—in some people—weight gain or cholesterol changes.
SNRIs
Serotonin-norepinephrine reuptake inhibitors (SNRIs), such as venlafaxine (Effexor) and duloxetine (Cymbalta), target two brain chemicals: serotonin and norepinephrine.
This dual mechanism can be useful for mood and anxiety symptoms tied to PTSD. The downside: some SNRIs also come with potentially pesky side effects like dry mouth, sleepiness, nausea, constipation, or hyperhidrosis, and more serious ones including raised blood pressure.
With SNRIs, it may also be harder to taper off than SSRIs, making careful monitoring important.
Prazosin
When PTSD hijacks your sleep, prazosin can be a game-changer. Originally used as a blood-pressure medication, it’s commonly used to treat PTSD-related nightmares and insomnia (issues that affect up to 70% of people with PTSD).
PTSD can trigger the release of norepinephrine, a stress hormone that can stimulate nightmares and nighttime hyperarousal. Prazosin interrupts this response at specific brain receptors, helping quiet the stress signal and improve sleep. Multiple studies support its effectiveness for reducing PTSD-related sleep issues.
What does “treatment-resistant PTSD” actually mean?
Brace yourself: the term sounds scarier (and more definitive) than it really is. In PTSD, conceptualizing someone as treatment-resistant “isn’t really helpful,” says Dr. Tahseen. “All it really means is that a treatment was tried and it didn’t achieve the goals.” That’s not a verdict on your ability to heal, and it’s definitely not a personal failure.
The term “treatment-resistant” originally comes from depression research and was meant to describe people who didn’t respond to two or more evidence-based treatments. In practice, it’s often used for administrative reasons like insurance approval for higher-cost meds or treatments that require closer monitoring, says Dr. Tahseen.
When it comes to PTSD, though, things get murky fast. There’s no single, agreed-upon definition. Some clinicians use the term after one unsuccessful evidence-based treatment; others after six months of therapy or medication at maximum tolerated doses. Some studies don’t define it clearly at all, just noting that symptoms persist despite care.
To make it even messier, there are no reliable predictors for who won’t respond to treatment. Research has suggested possible risk factors—like chronic trauma, early-life trauma, low social support, severe symptoms, comorbid mental health conditions, or poor physical health—but none of these are destiny.
PTSD looks wildly different from person to person, and treatments are highly individualized, says Dr. Tahseen. What works for one person may do very little for another. “It would make sense that some treatments would fail to make a difference for some people,” he explains.
So if you’ve heard—or feared—the phrase treatment-resistant PTSD, try not to let it get in your head. It doesn’t mean you’re stuck. It just means it’s time to try something different. And there are other options. Keep going. With the right approach, healing is absolutely still possible even if earlier attempts didn’t get you there.
Emerging and advanced PTSD treatments
When the usual PTSD treatment options fall short, the story doesn’t end there. If first- (or second-) line PTSD treatments haven’t helped enough, newer approaches are opening up more doors. From neuromodulation (aka brain-based) therapies to fast-acting medications and tech-assisted tools, these options are designed for people who haven’t gotten where they want to go with standard care. Some are already in use, others are still being studied, but many show real promise.
Neurofeedback
Imagine neurofeedback as a way of biohacking your brain activity. You wear a cap that reads your brainwaves and turns them into real-time visual or audio cues on a screen, helping you gradually learn how to regulate your own stress responses.
Prism for PTSD, an FDA-cleared device, zeroes in on the amygdala–prefrontal cortex circuit—the brain’s command center for fear and emotional regulation. PRISM has demonstrated significant response and remission rates within 8 weeks and the outcomes continue to improve over time for most people.
Meta-analyses suggest neurofeedback (like Prism) can reduce PTSD symptoms, along with related anxiety and depression, across different trauma backgrounds. A major bonus? Unlike exposure therapy, you don’t have to relive traumatic memories, which can make it feel more approachable for people who find revisiting trauma overwhelming.
TMS
Transcranial magnetic stimulation (TMS) is a non-invasive therapy using gentle magnetic pulses to stimulate specific areas of the brain. It’s already FDA-cleared for depression and other conditions, and it’s gaining traction as a PTSD treatment, too.
PTSD is linked to disrupted stress and fear-learning circuits, especially in the prefrontal cortex. TMS aims to help “reset” these networks so the brain can process stress more normally. Early data is promising: studies show both high- and low-frequency TMS can improve PTSD symptoms.
Like neurofeedback, TMS also offers a big upside: relief without having to rehash traumatic memories.
While side effects are usually mild—mostly headaches or scalp tingling—TMS is not a good fit for everyone. People with certain metal implants near the head or a history of seizures may not be able to receive TMS.
NightWare
Nightmares are one of the most stubborn and disruptive symptoms of PTSD. About 70% of people with PTSD experience frequent, persistent nightmares, which can linger even after treatment. These nightmares don’t just steal peace of mind; they fragment sleep, lower sleep quality, and leave people chronically under-rested. Furthermore, poor sleep quality worsens chronic health conditions (like high blood pressure) as well as mood regulation, focus, concentration and memory.
That’s where NightWare comes in. This FDA-cleared digital medical device is designed to reduce sleep disruption in psychiatric conditions like PTSD. Pairing special software with an Apple Watch, it tracks heart rate and movement during sleep to detect patterns that suggest a nightmare may be starting. When it does, the device delivers gentle vibration—enough to interrupt the nightmare without fully waking you—helping the brain shift out of distress and back toward more stable sleep.
In a qualitative study, people using NightWare reported better sleep quality and a clinically meaningful reduction—or even elimination—of nightmares related to PTSD and nightmare disorder.
Important caveat: this isn’t a standalone fix. NightWare is meant to be used alongside other PTSD treatments, not instead of them. Think of it as a sleep-supporting tool—one piece of a broader, personalized PTSD treatment plan.
Stellate ganglion block
For many people with PTSD, symptoms are driven by chronic hyperarousal—an always-on fight-flight-or-freeze response powered by an overactive sympathetic nervous system. Stellate ganglion block (SGB) aims to dial that system down, helping the body feel safer before the mind can follow.
So what is SGB, exactly? SGB is a brief, minimally invasive procedure that involves injecting a local anesthetic into a small cluster of nerves in the neck called the stellate ganglion, located on either side of the voice box. Essentially, it briefly “blocks” these nerves, interrupting the stress response. The procedure typically takes under 30 minutes, is considered low risk, and for some people, symptom relief shows up quickly.
In a study of military members with PTSD, over 70% of those who received a right-sided SGB experienced improvements in PTSD symptom scores lasting three to six months. Another study in civilian patients found that while a small group didn’t respond to a right-sided injection (4.4%), they improved after a left-sided SGB—hinting that both sides of the nervous system may be viable targets.
While more data is still needed on stellate ganglion block for PTSD, for certain people, it appears to meaningfully calm the body’s alarm system.
Ketamine and esketamine
When PTSD symptoms won’t budge, ketamine may offer another path forward. Originally developed as an anesthetic, ketamine has gained attention as a fast-acting treatment for depression, and more recently, as a potential option for PTSD, especially when symptoms have been stubbornly resistant to other care.
So how does ketamine actually help? While researchers are still piecing together the full picture, studies in both animals and humans suggest ketamine boosts neuroplasticity, or the brain’s ability to rewire itself. It also appears to increase activity in the prefrontal cortex, a key area involved in regulating fear and supporting fear extinction, which may help loosen trauma’s grip.
Several studies have found meaningful reductions in PTSD symptom severity (measured by PCL-5 scores) as early as 24 hours after the first ketamine infusion, with benefits lasting through treatment courses ranging from one to four weeks. For safety, ketamine is typically delivered via IV in a closely supervised clinical setting, where blood pressure, breathing, dissociation and overall safety can be monitored.
Esketamine
Esketamine—a nasal spray derived from ketamine and FDA-approved for treatment-resistant depression—is also showing promise for PTSD. In a small retrospective case series, all patients receiving esketamine alongside psychotherapy experienced clear reductions in PTSD symptoms, suggesting it may be especially helpful for treatment-resistant cases.
But ketamine and esketamine aren’t for everyone. More research is still needed to determine who benefits most and how best to use these therapies safely, particularly for people with a history of substance use or psychotic disorders. Used thoughtfully and under expert supervision, though, they may offer relief when other options haven’t.
Virtual reality exposure
Virtual reality (VR) takes traditional exposure therapy and turns the dial up on realism—without sacrificing safety. VR can recreate sights, sounds, and even smells or physical sensations linked to a traumatic experience, helping people approach memories they may have been avoiding. It sounds intense (because it is), but it’s done gradually, at a pace you can tolerate—you’re not thrown in the deep end. And, equally important, a trained clinician is always guiding you, supporting you as you process what comes up.
One VR exposure therapy system, BraveMind, creates immersive combat “worlds” designed for veterans with PTSD. By repeatedly revisiting trauma-related memories in a controlled, clinical environment, the brain’s stress response may soften, and the memories can lose some of their emotional punch. The goal isn’t to retraumatize—it’s to help the brain learn that these memories, while painful, aren’t dangerous anymore.
What does the research show so far? Though it’s still early, studies in military populations with PTSD are hopeful. Medical VR also hasn’t received an FDA label yet, though it remains an active area of review.
Keep in mind, most VR exposure research has focused on military service members, so results aren’t necessarily applicable for all trauma types. More studies are needed, especially trials using highly personalized virtual scenarios for non-combat trauma.
MDMA-assisted therapy
From rave to research lab? Yep. Best known as a party drug, MDMA (the main ingredient in molly or ecstasy) has been explored as a possible treatment for PTSD when paired with structured psychotherapy in a tightly-controlled clinical setting. Early results initially sparked real excitement, suggesting MDMA-assisted therapy might help people with PTSD.
Then came the record scratch. Those early hopes took a hit when major journals retracted later MDMA studies due to serious ethical violations. In August 2024, an FDA advisory panel overwhelmingly recommended against approving MDMA-assisted therapy for PTSD, citing flawed data and unresolved safety concerns.
So, where do things stand now? MDMA remains a Schedule I substance and is only available through approved research trials.
In case you’re thinking about trying MDMA on your own, don’t. Street MDMA is a hard no. Studies suggest only about 48% of what’s sold as “MDMA” actually contains what it claims, making unsupervised use both unpredictable and dangerous.
Even in controlled medical settings, MDMA isn’t risk-free. Potential side effects include cardiovascular issues and possible neurotoxicity, which is why close medical monitoring is non-negotiable.
Relief within reach
Care covered by your insurance
Radial provides advanced mental health treatment, covered by the insurance you already use.








Complementary therapies
Sometimes healing from PTSD means thinking a little outside the therapy box. Complementary therapies aren’t replacements for evidence-based treatment, but for many people, they’re powerful add-ons that help calm the nervous system, reconnect mind and body, and support healing in ways talk therapy alone can’t always reach.
Trauma-sensitive yoga
When words fall short, the body often speaks up. Trauma doesn’t just live in the mind—it can show up physically as chronic tension, pain, or a constant feeling of being on edge. Trauma-sensitive yoga is designed for exactly this reality.
Unlike traditional yoga, trauma-informed yoga focuses less on poses and more on awareness, choice, and safety. Instructors are specially trained to work with trauma survivors, offering multiple options, avoiding triggering positions, and emphasizing that you’re always in control of your body.
The payoff can be meaningful. One qualitative study found trauma-sensitive yoga helped participants regulate emotions, feel safe in their bodies again, and even experience growth beyond the mat, enhancing self-worth, agency, and connection to others. A 2023 meta-analysis reviewing 13 studies also found trauma-informed yoga to be a safe, effective therapeutic option for women with PTSD.
Acupuncture
Acupuncture might sound intimidating (all those needles!), but there’s growing evidence that it can support PTSD recovery, and not just in a “relaxation placebo” kind of way.
Emerging data suggests acupuncture may help regulate stress hormones, calm the nervous system, and even influence brain structure—all systems that tend to be out of sync in PTSD. In short, acupuncture may help create the conditions needed for deeper healing to take hold.
It’s not a standalone cure, but for some people, it’s a surprisingly effective piece of the larger treatment puzzle.
PTSD treatments to avoid
While research continues to expand the PTSD toolbox, there are a few approaches experts consistently advise against because they’re ineffective, risky, or can backfire over time.
Some medications and substances
Some meds may ease symptoms short-term, but aren’t a good long-term plan for PTSD, while others aren’t effective at all.
- Sleeping pills and benzodiazepines: These can offer brief relief for sleep or anxiety, but they come with a catch. They carry “a high risk of worsening PTSD over time if taken for too long,” says Dr. Tahseen. Dependence can occur, and they can worsen PTSD symptoms over time. Benzodiazepines can also interfere with your brain’s ability to benefit from psychotherapy.
- Atypical antipsychotics: These drugs have limited benefit for PTSD, plus they come with serious metabolic risks, including high blood sugar, diabetes, and heart disease.
- Certain anticonvulsants and related agents: Medications like valproate, lamotrigine, tiagabine, and partial NMDA receptor agonists (like d-cycloserine) haven’t shown strong or consistent benefits for PTSD.
- Cannabis: The 2023 VA/DoD PTSD Clinical Practice Guidelines recommend against cannabis for PTSD treatment. While some people use it hoping for relief, there isn’t enough data proving its efficacy, and it can potentially worsen symptoms, increase tolerance, and raise the risk of dependence.
Moving too fast in therapy
Healing isn’t a race, and pushing too hard can blow up in your face. Trauma-focused therapies can be powerful and life-changing, but faster isn’t always better. It’s understandable to want relief right now and dive in headfirst, but pacing matters, says Dr. Tahseen.
When it comes to many trauma therapies, going too fast can be counterproductive. These treatments often involve revisiting difficult memories, and doing too much too soon can feel overwhelming, re-traumatizing, or lead people to drop out altogether.
Dr. Tahseen has seen people try to tackle everything at once and “end up opening wounds too deep, very quickly,” he adds. Slow, steady progress isn’t a setback; it’s often exactly what makes healing sustainable.
A skilled therapist can guide you through the process to ensure proper pacing and that you have the necessary tools to manage what comes up during treatment without being totally overwhelmed.
How to find the right PTSD treatment and support for you
Real talk: Your PTSD provider matters more than you think. “Finding the right psychiatrist and/or psychotherapist is critical,” says Dr. Tahseen—and not just because they’re writing the prescriptions or running the sessions. The right provider can shape whether treatment actually helps or quietly stalls.
Step one: get the diagnosis right.
PTSD is often misdiagnosed or missed, says Dr. Tahseen. A skilled provider understands how many ways PTSD can show up and knows how to distinguish it from (or recognize when it overlaps with) anxiety, depression, or other conditions. That accuracy matters because the wrong diagnosis can send you down the wrong treatment path.
Next: build a treatment plan that fits your life.
PTSD doesn’t live in one neat box. It can affect sleep, work, relationships, physical health—everything, says Dr. Tahseen. A good provider takes time to understand where it hits hardest for you and uses that to shape a personalized plan.
They’ll also help decide which therapies make sense, knowing there’s no universal “best” option. “It’s not easy to know which psychotherapy will work,” says Dr. Tahseen. “A lot of effective treatment relies on finding a good psychotherapist.”
Then comes the real work—together.
Healing from PTSD isn’t linear, and you shouldn’t have to do it alone. The right provider knows how to pace treatment. “I’ve witnessed people driving towards addressing everything all at once and end up opening wounds too deep, very quickly,” says Dr. Tahseen. “It’s okay to take the healing slow and sometimes that’s necessary.”
Your therapist will also help you navigate setbacks and adjust when things feel overwhelming or stuck. They’re not just overseeing your care—they’re in the trenches with you.
Here’s the hard truth most people aren’t told. Not every therapist is trained to treat PTSD well. “What many patients don’t know is that most psychiatrists and psychotherapists do not have adequate experience working with post-traumatic diagnoses,” says Dr. Tahseen. When treatment doesn’t help, patients often blame themselves when the real issue is a lack of trauma-specific training, he adds. This isn’t meant to scare you, just to name a very common problem.
So how do you stack the odds in your favor? Start with referrals whenever possible—someone trusted, highly recommended, or known for trauma work, says Dr. Tahseen. And when you meet a new provider, remember: you’re allowed to interview them. Fit matters.
Use this quick cheat sheet when talking to a potential provider:
- Do you have experience treating trauma survivors or PTSD specifically?
- What evidence-based therapies do you use (like CPT, prolonged exposure, or EMDR)?
- Do you prescribe medications for PTSD, and if so, which ones?
- What insurance do you take, and what are the out-of-pocket costs?
Need help finding trauma-informed care? These directories can connect you with providers trained in evidence-based PTSD treatments:
- Cognitive processing therapy provider roster
- Prolonged exposure therapist locator – Emory University
- Center for the Treatment and Study of Anxiety (directory of therapists trained in prolonged exposure) – Penn Medicine
- EMDR International Association therapist locator
- International Society for Traumatic Stress Studies (ISTSS) clinician directory
- American Psychological Association (APA) psychologist locator
Finding a provider can take effort, but the right match can change everything.
The bottom line
PTSD can show up in countless ways, and that’s exactly why PTSD treatment has to be personal, flexible, and collaborative. From getting the diagnosis right to setting realistic goals, pacing therapy safely, and adjusting the plan when something isn’t working, effective care is about progress, not perfection.
If one approach doesn’t help, it doesn’t mean you’re broken or that healing isn’t possible. It just means it’s time to try something different. Many people experience meaningful relief, and remission is possible with the right combination of tools, timing, and guidance.
When you’re ready, support is here. Radial makes it easier to access fast-acting, evidence-based PTSD treatments without the guesswork. Connect with a licensed clinician virtually or in person who will take the time to understand your symptoms, your history, and your goals, and work with you to build a treatment plan that actually fits your life.
Key takeaways
- PTSD treatment works, but it’s highly individualized. What helps one person may not help another, and finding the right fit can take time.
- Psychotherapy is the backbone of effective care. Evidence-based, trauma-focused therapies like CPT, prolonged exposure, and CBT are first-line treatments.
- Medications can help manage symptoms, but they’re usually not enough on their own. They work best as part of a broader, personalized plan.
- “Treatment-resistant PTSD” doesn’t mean you won’t heal. It usually just means a particular approach wasn’t the right match.
- Newer treatment options (like neurofeedback or TMS) offer hope—especially when first-line treatments fall short.
Frequently asked questions (FAQs)
What is typically the best treatment for PTSD?
The short answer: those with the strongest evidence. And across clinical guidelines, psychotherapy is considered the backbone of PTSD treatment. According to the APA, first-line trauma-focused therapies include:
- Prolonged exposure (PE)
- Cognitive processing therapy (CPT)
- Cognitive behavioral therapy (CBT)
These approaches have the most consistent data for reducing PTSD symptoms. That said, the best treatment is the one that’s the right fit for you. If first-line therapies aren’t moving the needle, there are other effective options for treating PTSD. Don’t give up until you find something that works.
How does EMDR work?
Honestly? The science isn’t conclusive. What we do know is that EMDR works, even if the exact brain mechanism is still debated.
Here’s what to expect during EMDR sessions: you bring up distressing memories while following a rhythmic, back-and-forth stimulus—such as moving lights, tapping, or sounds. This “bilateral stimulation” appears to help the brain reprocess and re-store traumatic memories, reducing how emotionally intense they feel over time. Think of it less as erasing the memory and more as turning down its volume.
What is the success rate of PTSD treatment?
It depends on the treatment and how success is defined. Different PTSD treatments show different response and remission rates, and many people improve without becoming completely symptom-free. Some examples:
- In one study of people who completed cognitive behavioral therapy (CBT) for PTSD, 67% no longer met diagnostic criteria after treatment.
- A meta-analysis of randomized controlled trials found about 50–60% of people responded to sertraline, an SSRI commonly used for PTSD. Response generally means a 50% symptom decrease.
- In one study combining psychoeducation, physical activity, prolonged exposure, and EMDR, 75.8% of treatment completers no longer met PTSD criteria after treatment. That said, recovery wasn’t always “perfect”: over half still reported some lingering symptoms (like avoidance or intrusive memories) six months later.
Deep dive recommendations:
- The Frontier Psychiatrists Podcast. PRISM: Trauma Treatment You Don’t Need to Talk About. https://podcasts.apple.com/us/podcast/prism-trauma-treatment-you-dont-need-to-talk-about/id1577248149?i=1000666244010
- Psychiatry & Psychotherapy Podcast. Episode 220: Writing to Overcome Trauma and Improve you Mental Health. https://podcasts.apple.com/us/podcast/220-writing-to-overcome-trauma-and-improve-your/id1335892956?i=1000666402206
- Psychiatry & Psychotherapy Podcast. Episode 209: PTSD and Cognitive Processing Therapy with Patricia Resick. https://podcasts.apple.com/us/podcast/209-ptsd-and-cognitive-processing-therapy-with/id1335892956?i=1000650875608
- Psychiatry & Psychotherapy Podcast. Episode 203: Adverse Childhood Experiences and Their Lasting Impact on Health: A Comprehensive Guide. https://podcasts.apple.com/us/podcast/203-adverse-childhood-experiences-and-their-lasting/id1335892956?i=1000642249665
- Psychiatry & Psychotherapy Podcast. Episode 204: Adverse Childhood Experiences Part 2: Measurement, Impact on Future Mental Health, Dissociate, and Timing of Trauma. https://podcasts.apple.com/us/podcast/204-adverse-childhood-experiences-part-2-measurement/id1335892956?i=1000643970883
- Psychiatry & Psychotherapy Podcast. Episode 217: Adverse Childhood Experiences - HPA axis & Brain changes: cortisol, amygdala, hippocampus, cytokines, & epigenetics (Part 3 of ACE series). https://podcasts.apple.com/us/podcast/217-adverse-childhood-experiences-hpa-axis-brain-changes/id1335892956?i=1000662773245
- Psychiatry & Psychotherapy Podcast. Episode 55: How to Pick A Good Therapist. https://podcasts.apple.com/us/podcast/055-how-to-pick-a-good-therapist/id1335892956?i=1000446598404
- Psychiatry & Psychotherapy Podcast. Episode 48: The Unspeakable Mind: Stories of Trauma and Healing from the Frontline of PTSD Science with Dr. Shaili Jain. https://podcasts.apple.com/us/podcast/048-the-unspeakable-mind-stories-of-trauma-and/id1335892956?i=1000441364279
Editorial Standards
At Radial, we believe better health starts with trusted information. Our mission is to empower readers with accurate, accessible, and compassionate content rooted in evidence-based research and reviewed by qualified medical professionals. We’re committed to ensuring the quality and trustworthiness of our content and editorial process–and providing information that is up-to-date, accurate, and relies on evidence-based research and peer-reviewed journals. Learn more about our editorial process.
Let's connect
Get started with finding the right treatment for you or someone you care about
Get startedExplore more posts




