Treatment for Postpartum Depression: How to Find Relief

Postpartum depression is highly treatable, but knowing where to start can feel like a lot. Treatment for postpartum depression begins with understanding your options, how quickly they work, what the process looks like, and how to find the right fit for you.
Treatment for postpartum depression might not be something you expected to be Googling, but here you are. Maybe you’re feeling persistently sad, anxious, numb, or on edge. Maybe you’re having thoughts that scare you. Or maybe you just don’t feel like yourself and can’t stop wondering: Is this normal … or do I need help?
You’re not alone. After a complicated pregnancy and scary birth, I thought the hardest part was behind me. Then postpartum depression hit, and everything felt heavy. I felt guilty for not “enjoying” those early moments with my baby. Days and nights blurred together in a fog of feedings, exhaustion, and darkness I couldn’t seem to shake.
What changed things? Getting real postpartum depression help—including working with a therapist who specialized in postpartum mental health. Recovery wasn’t instant, but slowly, I started finding glimmers of light again. That’s what postpartum depression recovery can look like: not perfect, not overnight, but absolutely possible.
In this guide, we’ll walk through what postpartum depression is (and isn’t), compare postpartum depression therapies, medications, and newer non-drug options, and explain how to choose the right treatment based on your symptoms, breastfeeding status, and needs. Whether you’re actively dealing with postpartum depression or supporting someone who is, this is your starting point.
Healing happens through strong relationships
Compassionate, experienced mental health professionals focused on evidence-based care




What is postpartum depression, and how is it different from ‘baby blues’?
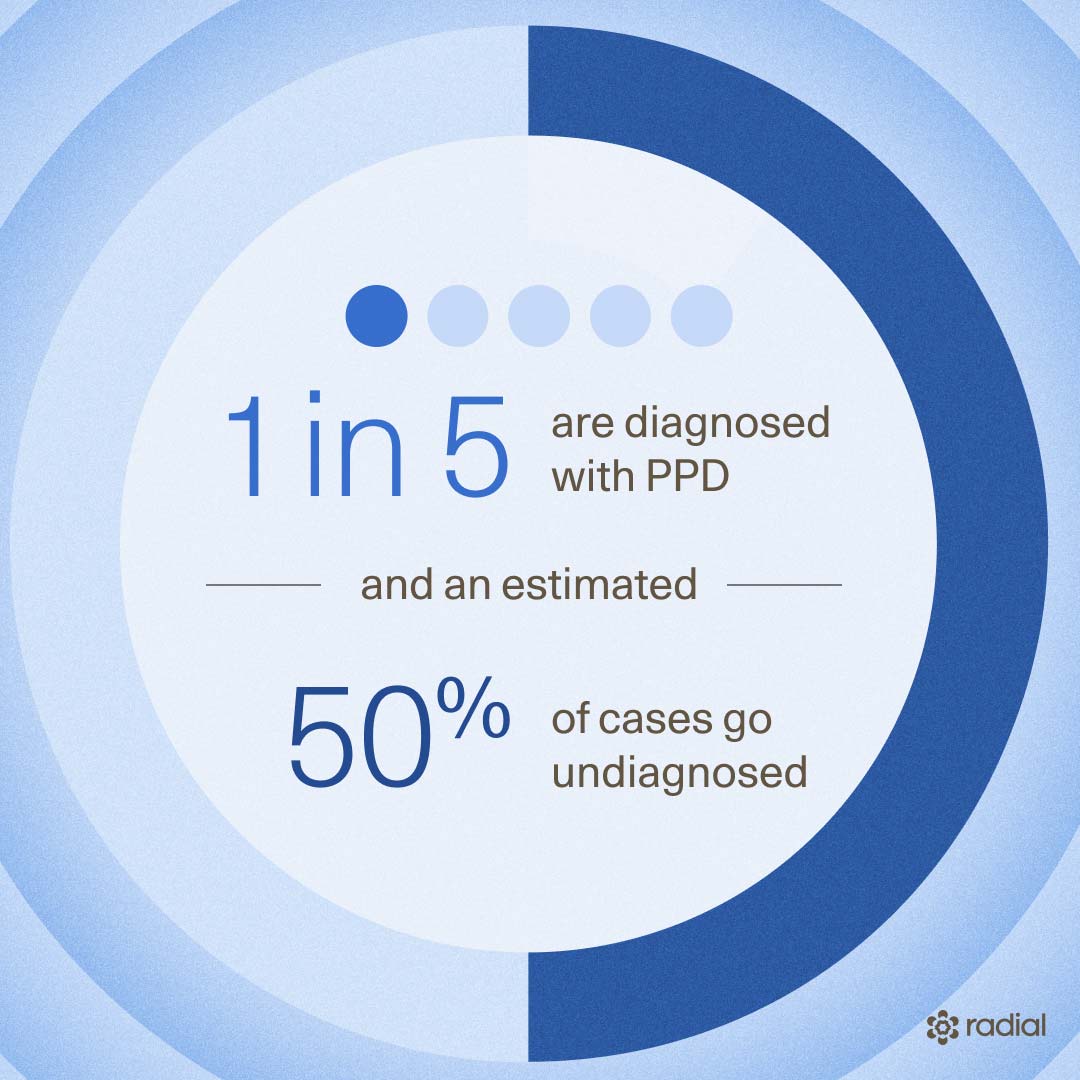
Postpartum depression (PPD) is the most common postpartum mood disorder, affecting approximately one in five women. But many cases go undiagnosed (up to 50 percent), often because stigma makes people hesitant to speak up about what they’re experiencing.
It impacts anyone (even those with uncomplicated birth experiences) and extends beyond typical mood swings.
PPD can feel like persistent sadness, hopelessness, and loss of interest or joy. You might also notice changes in sleep or appetite, low energy, irritability, trouble focusing, or even thoughts of self-harm or suicide.
To put that in context, it’s often confused with the far more common “baby blues.” The baby blues are short-lived and milder, usually peaking in the first few days after birth and easing up within two weeks. PPD, by contrast, lasts longer, feels more intense, and often requires treatment.
At the other end of the spectrum is a much rarer—but more severe—condition. Postpartum psychosis can involve hallucinations, delusions, and disorganized thinking, and requires immediate medical care due to safety risks for both parent and baby.
If you have urgent symptoms, do not wait. Red flags include: suicidal thoughts, delusions, or hallucinations (like hearing voices telling you to harm your baby)
How is postpartum depression treated?
The good news: postpartum depression is highly treatable, and you have options. But PPD treatment isn’t one-size-fits-all. What you’re offered will depend on how severe your symptoms are, what feels right to you, and practical considerations—like whether you’re breastfeeding or concerned about medication side effects.
From talk therapy to fast-acting medical options, here’s what actually works:
- Therapy: Evidence-based approaches like cognitive behavioral therapy (CBT) and interpersonal psychotherapy (IPT) are often the first step, especially for milder symptoms. They can help you build coping skills, shift unhelpful thought patterns, and improve communication and support.
- Antidepressants: Medications—most commonly selective serotonin reuptake inhibitors (SSRIs)—are a frontline treatment, says Sarah Quaratella, MD, a board-certified psychiatrist who specializes in women's mental health and reproductive psychiatry. They work by increasing serotonin, a brain chemical that helps regulate mood, sleep, and stress.
- Neuromodulation: These treatments “tune” brain activity using targeted energy, like magnetic pulses or electrical stimulation. One option, transcranial magnetic stimulation (TMS), is gaining traction as a non-drug approach for perinatal depression.
- Rapid-acting options: When symptoms are severe—or not improving with other treatments—faster-acting interventions may be used. These include medications like zuranolone, as well as electroconvulsive therapy (ECT), which can reduce symptoms in days rather than weeks.
In general, therapy may be enough for milder cases, while medication or faster-acting postpartum depression treatments come into play when symptoms are more severe or urgent.
Therapy for postpartum depression
Therapy is often the first-line treatment for mild to moderate postpartum depression. These approaches are well-studied, effective, and tailored to help you navigate both the emotional and relational upheaval that can come with new parenthood.
The most common, evidence-based postpartum depression therapy approaches include:
- CBT (cognitive behavioral therapy): Helps you spot and shift unhelpful thought patterns. You’ll learn practical tools—like coping strategies, problem-solving skills, and relaxation techniques—to manage stress and improve mood.
- IPT (interpersonal psychotherapy): Focuses on relationships—because who (and how) you connect with matters. It helps you work through conflict, improve communication, and strengthen your support system.
- Group psychotherapy: Think: structured support with people who get it. Group therapy can reduce depression and anxiety symptoms while creating a sense of community, validation, and shared experience.
Who it's best for:
- For people with mild to moderate postpartum depression
- For people who prefer to avoid medication
How long it takes to work:
Therapy takes time, but it works. In studies of CBT and IPT, many people start to notice improvement around 8 weeks.
Pros:
- Offers a safe, supportive space to process emotions
- No medication side effects, making it compatible with breastfeeding
- CBT can often be done online, improving access and convenience
Cons:
- Takes several weeks to feel the full benefit
- May not be enough on its own for more severe symptoms
- Access can be a barrier—cost, insurance coverage, and availability of specialized postpartum care can all limit options
The takeway: Therapy is a powerful first step, but it’s not the only one. It’s often the foundation of treatment and an essential piece of the puzzle. But if symptoms are severe or interfering with daily functioning, you may need additional support or a treatment that works more quickly.
Conventional medication for postpartum depression
When symptoms go beyond what therapy alone can handle, antidepressants for postpartum depression are commonly used. The go-to meds are often selective serotonin reuptake inhibitors (SSRIs). These “are the first-line pharmacological treatment with the strongest evidence base,” says Dr. Quaratella.
These drugs work by increasing levels of serotonin, a brain chemical that helps regulate mood. “Sertraline (Zoloft) is the most studied and often recommended,” Dr. Quaratella notes, because it has “low transfer into breast milk,” a strong safety profile, and solid “efficacy data specific to PPD.”
SNRIs (like venlafaxine) can be a good alternative if SSRIs don’t work though they may increase anxiety for some people (though there isn’t much data to support this), says Dr. Quaratella.
Who it's best for:
- People experiencing moderate to severe symptoms that interfere with daily functioning
- People who've responded well to antidepressants before or prefer a medication-based approach
How long it takes to work:
This is a slow build, not a quick fix. It can take time to find the right medication, which may require trying more than one type. Antidepressants don’t work immediately—most people feel the full effects after about 4–6 weeks (sometimes longer).
Pros:
- Can reduce depressive symptoms (some research shows higher response and remission rates compared to placebo)
- Widely available and commonly prescribed
- Can be combined with therapy for a stronger overall effect (some studies suggest meds plus therapy are more effective than either approach on its own)
- Some options are considered compatible with breastfeeding
Cons:
- Side effects of SSRIs can include nausea, insomnia, drowsiness, headache, agitation, and decreased sex drive
- Finding the right medication and dose can take trial and error
- It takes several weeks to feel the full benefits
- There's potential for drug interactions
- Small amounts can pass into breast milk and potentially affect the baby
- Some people experience withdrawal-like symptoms when stopping, especially after long-term use
- Research specific to postpartum depression is still somewhat limited, and results on effectiveness are mixed
The takeaway: Antidepressants are often effective for moderate to severe postpartum depression, particularly when you need more support than therapy alone can provide. Just know: they take time to work, and finding the right fit may require some fine-tuning.
“No antidepressant has proven definitively superior in head-to-head PPD trials,” says Dr. Quaratella. In practice, the “best” option usually comes down to how well you tolerate it and your individual symptom profile—not major differences in effectiveness, she adds.
If you’ve been taking an antidepressant for 4–6 weeks without noticeable improvement—or if side effects feel unmanageable—it may be time to adjust the dose, switch medications, or consider a different treatment approach. Antidepressants don’t work for everyone, but there are other effective options.
TMS for postpartum depression
Transcranial magnetic stimulation (TMS) delivers magnetic pulses to specific areas of the brain through a device placed on the scalp, helping “reset” neural activity linked to mood regulation. TMS is already FDA-approved for major depression and shows promise as a non-drug option for postpartum depression.
Who it's best for:
- Those who haven’t responded to other treatments
- Those who have moderate to severe symptoms
- Those who've had significant side effects from medication or prefer to avoid it
How long it takes to work:
- Standard TMS typically involves daily sessions over 6–8 weeks
- Accelerated protocols like SAINT or intermittent theta burst stimulation (iTBS) deliver a higher “dose” in less time, with small studies showing improvement in as little as two weeks
Standout box: At the time of publication, there are clinical trials of SAINT for postpartum depression that are currently enrolling participants. Click here to learn more.
Pros:
- A solid alternative if medication hasn’t worked or isn’t your preference
- Noninvasive and drug-free, so no medication exposure for parent or baby
- Evidence suggests lasting improvements in depression and anxiety symptoms
- Generally well tolerated, with mild side effects like headache or scalp discomfort
Cons:
- Standard treatment requires a significant time commitment (daily sessions for weeks)
- Accelerated options like iTBS aren’t widely available yet or covered by insurance
- Research for TMS in postpartum depression is still limited (though early results are promising)
- Very low risk of seizure—the most serious, but rare, side effect of TMS
The takeaway: TMS therapy for postpartum depression is promising, but still emerging. It appears to be safe and well tolerated, and early results suggest it can be effective, especially for people who haven’t responded to medication or don’t want to take it. Larger, more rigorous studies are still needed, but for now, it’s a compelling alternative with cautious optimism behind it.
Rapid-acting treatments for postpartum depression
When you need relief fast, there are options. If symptoms are severe, worsening, or pose safety risks, faster-acting treatments may be necessary. These options are designed to work quickly—sometimes in days.
Electroconvulsive therapy (ECT)
ECT is a form of neuromodulation that uses controlled electrical stimulation (under anesthesia) to trigger a brief, therapeutic seizure.
Who it’s best for:
- People with severe or life-threatening symptoms
- People who've had suicidal thoughts or acute psychosis
- Those with depression that hasn’t improved with other treatments
How long it takes to work:
- Typically 6–12 sessions over 2–4 weeks, with some people improving within the first week
Pros:
- High response (70%) and remission (50-60 %) rates for severe depression
- Often more effective than medication alone in severe cases
- May work even better in the postpartum period
- Compatible with breastfeeding
Cons:
- Requires treatment in a medical setting
- Often misunderstood or stigmatized
- Temporary side effects like short-term memory issues
Zuranolone
Zuranolone (aka the postpartum depression pill) is a newer, FDA-approved neurosteroid specifically for postpartum depression. It’s a daily pill taken for two weeks that acts on GABA-A receptors (not serotonin), helping regulate mood through a different pathway. It works similarly to brexanolone—the first FDA-approved medication for PPD, delivered as a 60-hour IV hospital infusion—which was recently discontinued due to the logistical hurdles of treatment.
Who it’s best for:
- People with severe or life-threatening symptoms
- People who've had suicidal thoughts or acute psychosis
- Those with depression that hasn’t improved with other treatments
How long it takes to work:
Some people respond within days—about 25% by day 3, 50% by day 8, and almost 60% by the end of treatment
Pros:
- Can improve symptoms within days
- Generally well tolerated
- Short, outpatient treatment (just two weeks)
Cons:
- Limited access and can be expensive
- Not recommended during breastfeeding due to limited safety data
- Side effects may include drowsiness, dizziness, headache, and sedation
- Requires careful monitoring
Ketamine/esketamine
Originally used as anesthetics, ketamine and esketamine are now being studied for rapid depression relief (including postpartum depression). Esketamine (brand name Spravato), a nasal spray, is FDA-approved for treatment-resistant depression.
Who they're best for:
- People with severe or life-threatening symptoms
- People who've had suicidal thoughts or acute psychosis
- Those with depression that hasn’t improved with other treatments
How long it takes to work:
- Effects can begin within hours to days
Pros:
- Extremely rapid relief
- May help even if other antidepressants haven’t worked
- Early research shows promise for both short- and longer-term symptom reduction of postpartum depression
- Appears to pose very low risk to breastfed babies
Cons:
- Effects can be short-lived (peaking after 24-48 hours of use and typically lasting for two weeks)
- Side effects may include dizziness, blurred vision, headache, or dissociation
- Must be given in a clinical setting for monitoring
- Coverage can be limited (ketamine is often off-label; esketamine may not be covered for postpartum depression)
The takeaway: Fast-acting treatments can be game-changing, particularly in urgent situations. They can be life-saving for people with severe symptoms, but they also come with tradeoffs, so it’s important to weigh the risks and benefits with your provider—especially compared to the very real risks of leaving postpartum depression untreated.
How to choose the right PPD treatment for you
Not all postpartum depression looks the same, so treatment shouldn’t either. The right approach to treating postpartum depression depends mostly on how severe your symptoms are and how quickly you need relief. “Symptom severity is the primary variable,” says Dr. Quaratella. It’s “determined by the frequency, intensity, and duration of depressive symptoms.”
From there, your preferences, support system, and comfort with different treatments help shape the plan as well.
Here’s how to think about your options based on what you’re experiencing:
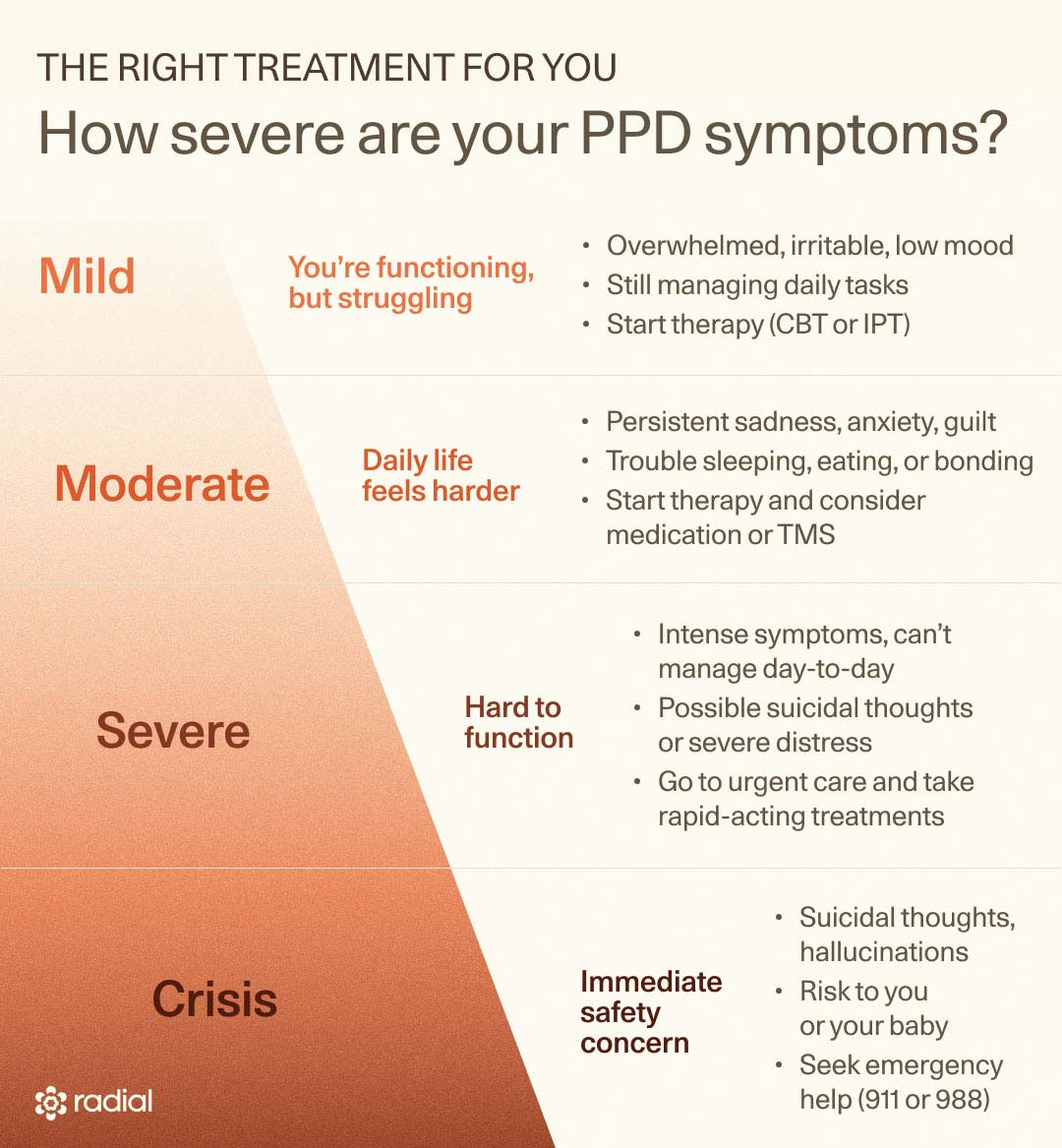
If your symptoms are mild (you’re functioning, but struggling)
Mild postpartum depression usually means symptoms are there but still somewhat manageable. You can get through daily tasks and care for your baby, but it may feel harder than it should. You might feel overwhelmed, irritable, sad, anxious, or just not as connected or present.
What to start with: Postpartum depression is typically diagnosed when symptoms last at least two weeks. “Mild to moderate symptoms can often be addressed with psychotherapy alone, particularly CBT or interpersonal therapy (IPT),” says Dr. Quaratella.
Support matters: Sleep, practical help with the baby, and a solid support system can make a real difference (sleep deprivation and low support are key risk factors).
Timeline: Therapy takes time—most people start to notice improvement around 8 weeks.
If symptoms stick around or you’re not improving, it may be time to consider medication or neuromodulation
If your symptoms are moderate (daily life is getting harder)
Moderate postpartum depression is a step up in intensity. Daily life starts to feel like a real struggle. Sadness and anxiety may feel heavier and more constant, along with guilt or feelings of worthlessness. Things like eating, sleeping, or bonding with your baby can become noticeably harder.
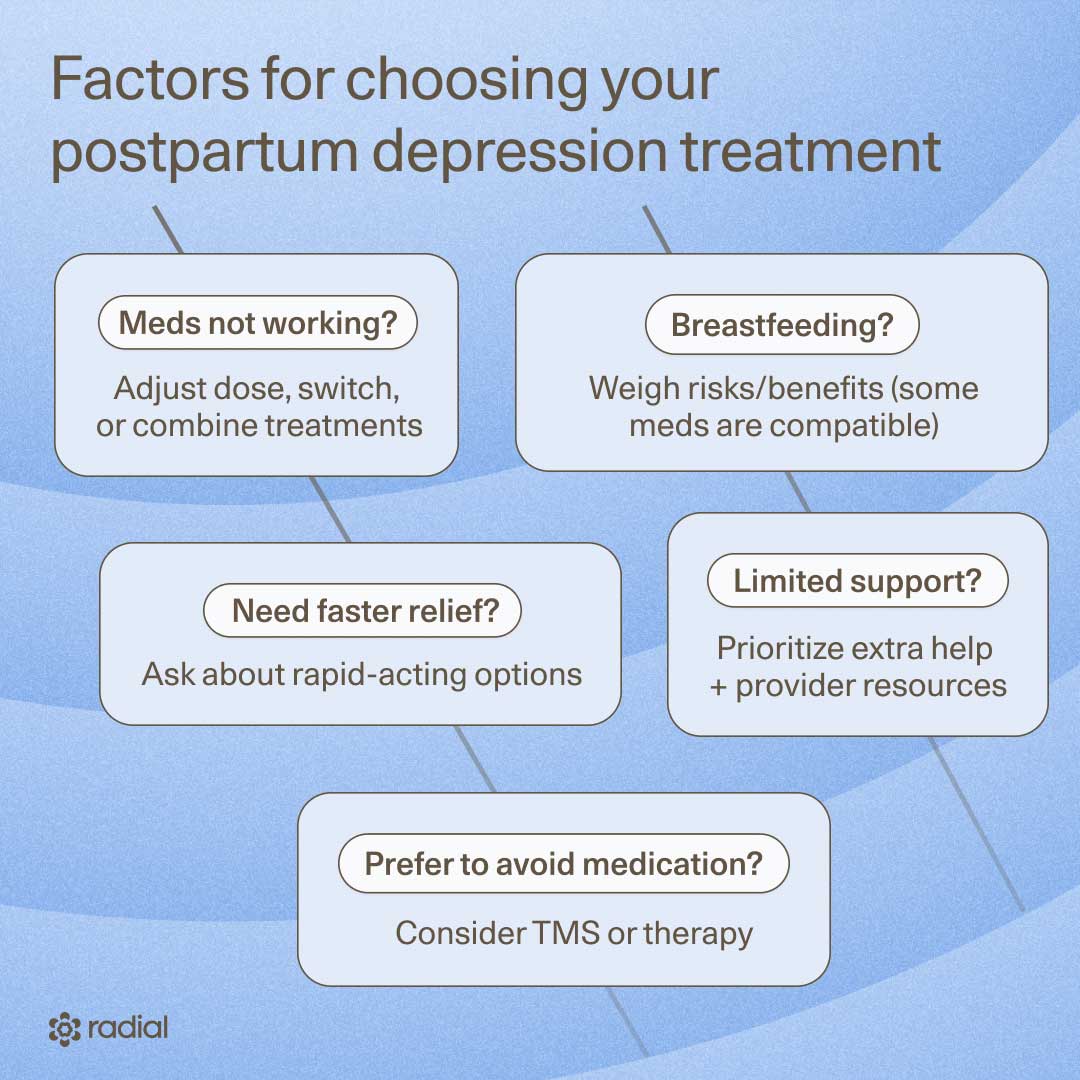
What to start with: “Moderate to severe symptoms are best treated with a combination of medication and therapy,” says Dr. Quaratella.
Prefer to avoid medication? Neuromodulation options like TMS may be worth considering.
Timeline: Still not instant—antidepressants typically take 4–6 weeks to reach full effect. Standard TMS takes about 6–8 weeks, though accelerated options may start to work in as little as two weeks.
If your symptoms are severe (you feel overwhelmed or unable to function)
Severe postpartum depression may include suicidal thoughts, psychosis, or an inability to function day to day, says Dr. Quaratella. These cases are urgent and require immediate medical evaluation, she adds.
What to do now: Contact your provider or go to the nearest ER for immediate care.
Treatment: When fast relief is critical, rapid-acting options like electroconvulsive therapy (ECT) or medications like zuranolone or ketamine may be recommended.
Timeline: ECT can start working within 1–2 weeks; zuranolone and ketamine may improve symptoms within days.
Other factors that affect your treatment choice
While symptom severity is the biggest driver of treatment decisions, it’s not the only one. Your preferences, medical history, and day-to-day realities all shape what’s safest, most practical, and most effective for you.
Here are a few key factors that can influence the plan, according to Dr. Quaratella:
- Breastfeeding plans: Some SSRIs are considered compatible with breastfeeding, and non-drug options like therapy and TMS are safer. Other treatments—like zuranolone—aren’t recommended while breastfeeding.
- Past treatment response: If SSRIs haven’t worked for you before, other options—like zuranolone or neuromodulation—may be a better fit.
- Anxiety alongside depression: Some medications (including SSRIs) can temporarily increase anxiety in the first few weeks, which can make sticking with treatment harder.
- Access and cost: Faster-acting treatments (like zuranolone or accelerated TMS) may be harder to access or more expensive.
- Ruling out other conditions: Postpartum thyroiditis can look like depression, so basic labs (like TSH) are often part of the workup.
- Your support system: Limited support can worsen symptoms, so providers should factor this in and help connect you with resources.
Postpartum depression treatment while breastfeeding: What to know
If you’re breast- or chestfeeding, it’s normal to have questions about how treatment—especially postpartum depression medication—might affect your baby.
Here’s the thing: many medications do pass into breast milk, but in very small amounts. “All psychotropic medications pass into breast milk to some degree, but detectable does not mean harmful,” says Dr. Quaratella.
What matters most is something called relative infant dose (RID), she says. Think of RID as the exposure snapshot. It estimates how much of the medication your baby gets through breast milk compared to your dose. In general, an RID below 10% is considered acceptable, says Dr. Quaratella.
Here’s how some common antidepressants compare, per Dr. Quaratella:
- Sertraline: RID ~0.5-3% (often the first choice)
- Paroxetine: Also low RID, but may carry a higher risk of withdrawal symptoms if stopped
- Fluoxetine: Higher RID (up to ~6-10% or more), making it less preferred
Newer medications like zuranolone don’t yet have enough safety data, so breastfeeding is typically not recommended during treatment.
Prefer to avoid medication? You still have options. Non-drug treatments like therapy and transcranial magnetic stimulation (TMS) can be effective and don’t involve medication exposure through breast milk.
This is a big decision, and you don’t have to figure it out alone. Choosing a treatment while breastfeeding is personal, and your provider can help you weigh the benefits and risks based on your specific situation. Tools like LactMed (NIH) and MotherToBaby offer reliable, evidence-based info about medications and breastfeeding if you want to dig deeper.
And one important reality check: “The decision to initiate medication must be weighed against the risk of not treating,” says Dr. Quaratella. Untreated postpartum depression can affect bonding and a baby’s development, so supporting your mental health is part of supporting your baby, too.
What you can do today (next steps)
When you’re in the thick of postpartum depression, everything can feel overwhelming. You might know you need help, but figuring out where to start can feel like too much.
Take a breath. You don’t have to solve everything today, just take one small step.
Here are a few low-lift ways to get started right now:
- Reach out to Postpartum Support International (PSI): Call or text 1-800-944-4773. It’s a “lower-barrier” way to connect with someone who specializes in postpartum depression, says Dr. Quaratella.
- Tell one person you trust: Reach out to a partner, friend, or family member to say you're struggling. Just saying it out loud can ease the isolation, help you feel less alone, and “creates accountability as you seek care,” says Dr. Quaratella.
- Contact your OB-GYN or midwife: Use the word depression. “They’re often the fastest path to evaluation and treatment,” says Dr. Quaratella. If calling feels like too much, a patient portal message works too (as long as symptoms aren’t severe), she adds.
- Do one small thing for yourself: Ask for help with a feeding so you can rest, step outside for a few minutes, or take a short walk, says Dr. Quaratella.
- Browse PSI’s provider directory: You can filter for therapists and psychiatrists specifically trained in postpartum depression, says Dr. Quaratella. No need to reach out or book anything yet; this is just a gentle first step to see that there are real people, in your area, ready to help when you’re ready.
- Check out Radial: Explore evidence-based treatments, including options for people who haven’t found relief with traditional care. You can book virtual consults in multiple states or access in-person treatment at select centers.
The bottom line
Postpartum depression can make everything feel heavy, confusing, and isolating, but it’s not permanent, and it’s not a reflection of who you are as a parent. With the right support and treatment, things can get better.
Have patience with yourself. You’re navigating a massive physical, emotional, and hormonal shift, and asking for help is not a failure—it’s a turning point.
Start small, but start somewhere. Whether that’s telling someone how you’re feeling, reaching out to your provider, or exploring your treatment options—you don’t have to figure it all out today. Just take the next step.
If you’re ready for more support, Radial can help you access the latest fast-acting, evidence-based treatments for postpartum depression. You can connect with a licensed clinician—virtually or in person—who will listen, understand your situation, and help build a treatment plan that works for you.
Key takeaways
- Postpartum depression is common and treatable. It’s more than “baby blues” and may need real support to improve.
- Treatment isn’t one-size-fits-all. Options include therapy, medication, neuromodulation, and faster-acting interventions for severe cases (or some combo of approaches).The right approach depends on your symptoms, preferences, and situation (including breastfeeding and urgency).
- Most treatments take time, but some options can work in days if symptoms are severe or not improving.
- If something isn’t working, you’re not stuck—adjusting, combining, or switching treatments is part of the process
Frequently asked questions (FAQs)
How long can postpartum depression last?
Short answer: it varies—a lot. Postpartum depression doesn’t follow a set timeline. For some people, symptoms last a few months (around 3 to 6 months). For others, they can stick around much longer (especially without treatment). In one study, about a quarter still had elevated symptoms three years postpartum.
What happens if postpartum depression is left untreated?
Untreated postpartum depression can make it harder to care for yourself and your baby, and the effects can be serious and long-lasting:
- Higher risk of suicide
- Difficulty with lactation
- Challenges with bonding and connection
- Potential impacts on your child’s cognitive, emotional, and behavioral development
What this means for you: early support matters. Getting help sooner rather than later can make a meaningful difference for both you and your baby.
Are antidepressants safe while breastfeeding?
With the right guidance, taking an antidepressant while breastfeeding can be a safe and effective part of your treatment plan.
Most antidepressants do pass into breast milk, but usually in very small amounts. One helpful metric is the relative infant dose (RID)—it estimates how much of the medication your baby is exposed to through breast milk. In general, an RID under 10% is considered acceptable, says Dr. Quaratella.
Editorial Standards
At Radial, we believe better health starts with trusted information. Our mission is to empower readers with accurate, accessible, and compassionate content rooted in evidence-based research and reviewed by qualified medical professionals. We’re committed to ensuring the quality and trustworthiness of our content and editorial process–and providing information that is up-to-date, accurate, and relies on evidence-based research and peer-reviewed journals. Learn more about our editorial process.
Let's connect
Get started with finding the right treatment for you or someone you care about
Get startedExplore more posts