OCD Treatment: What Works, What Doesn’t, and What’s New

OCD treatment isn't one-size-fits-all. Care starts with first-line treatments—the “go-to” options that providers recommend trying first because they have a strong track record of effectiveness. However, second-, third-, and even emerging options can also help if needed, especially if you haven’t responded well to other treatments. It's important to work with your doctor to find the approach that works for you.
Figuring out how to find the right treatment can be tough, but it can be particularly challenging when you have a condition that requires specialized treatment, like OCD. You might start reading about the different options and feel overwhelmed by all the jargon and acronyms. ERP? CBT? TMS? What does it all mean, and how can you make clear decisions about what will work best for your needs?
The most important thing to know as you begin your search is that obsessive-compulsive disorder is highly treatable, even when symptoms feel severe or you’ve had them for a long time. There isn’t a single "right" treatment that works for everyone. Instead, care typically follows a stepped process that is personalized for you based on the severity of your symptoms, the treatments you’ve tried in the past, and other individual needs.
In this article, we'll walk through the evidence-based treatment options, how they compare, and when they can be combined. We'll also explain what treatment-resistant OCD means, how clinicians decide what to try next, and how you can advocate for yourself to get appropriate, effective care.
How is OCD treated?
Obsessive-compulsive disorder, or OCD, is a mental health condition where people experience intrusive, unwanted obsessions that often lead to repetitive behaviors known as compulsions. These thoughts and behaviors often focus on specific themes, which can be grouped into different subtypes such as contamination OCD (fear of germs) and harm OCD (fear of hurting someone).
Some OCD subtypes can involve concerns about cleanliness, order, or precision that can overlap with obsessive compulsive personality traits or obsessive compulsive personality disorder (OCPD), which is sometimes why the label is sometimes misapplied in everyday language.
In OCD, intrusive thoughts and the compulsive behaviors used to relieve them create a repetitive cycle. This cycle is time-consuming, distressing, and hard to control. That distinguishes it from a preference for order or perfection that feels consistent with one’s personality.
"The problem is that the more we engage this cycle, the stronger it becomes," explains Dr. MaryEllen Eller, MD, the southeast regional medical director at Radial.
It follows a predictable pattern:
- An intrusive thought creates anxiety
- Anxiety leads to a compulsion
- Engaging in a compulsive behavior brings brief relief
- That momentary relief triggers the urge to respond the same way next time an anxious, intrusive thought happens
It’s a hard cycle to break because every time a person engages in a behavior to alleviate the anxiety caused by obsessive thoughts, it reinforces that OCD circuit. It's a cycle that, over time, becomes increasingly tough to manage.

Treatments help break this cycle, but it’s important to start by understanding how severe symptoms are and how much they interfere with quality of life, impact functioning, or cause impairment so clinicians can track how people are responding to treatment. To do this, clinicians often use a tool known as the Yale-Brown Obsessive Compulsive Scale, or Y-BOCS. It helps them understand how much time OCD takes up, how distressing it is, and how much it interferes with a person's life.
When it comes to treatment, the options that are usually recommended for some other conditions aren’t the best choice here. For example, talk therapy can sometimes make matters worse by validating a person’s irrational fears or inadvertently reinforcing the compulsions that keep the OCD cycle going. Instead, OCD is better treated with specialized options that have been shown to help break the cycle and reduce obsessive thoughts and compulsive behaviors.
What’s confusing for many people is the number of options available and figuring out which ones you should try first. Knowing which ones are right for you depends on a variety of factors, including your symptoms, your treatment history, and the evidence base behind certain approaches.
When you hear clinicians talk about first-, second-, and third-line treatments, they are referring to the order in which evidence-based treatments are typically tried. First-line treatments are those with the strongest evidence. That’s why clinicians typically recommend them first. Then, if symptoms don’t improve or if additional support is needed, they might suggest other approaches.
First-line OCD treatments (start here)
For most people, a treatment plan for OCD will start with the first-line approaches that have the best track record for reducing symptoms. Clinicians recommend these options first for a reason: they often focus on targeting the source–OCD cycle itself. The good news is that these approaches are often helpful, even if symptoms are severe. However, OCD is a chronic condition. Treatment often leads to reductions in symptoms and meaningful improvements in functioning rather than full remission, so people may continue to experience some symptoms over time.
CBT with ERP
Exposure and response prevention (ERP) therapy is a type of cognitive-behavioral therapy that is often considered the gold standard for treating OCD. It can help people gradually face their fears while resisting the urge to engage in compulsive behavior.
"ERP trains the brain to be 'ok’ with the anxiety caused by the intrusive thoughts," Dr. Eller explains. While it may seem counterintuitive, not reacting to anxious thoughts teaches the brain that things will be fine–even if the feared scenario does happen. "If we can be 'ok' if the worst were to happen, then we can definitely deal with what's happening in the moment," Dr. Eller says. It gradually lessens the power that intrusive thoughts have, and obsessions and compulsions begin to fade.
While ERP therapy is typically the "go-to" option, that doesn't mean it's right for everyone. Facing your fears can be uncomfortable, and not everyone is ready or able to tolerate it.
There are also other challenges that make ERP less accessible. For example, people in rural areas may struggle to find clinicians trained in ERP. “Finding a qualified ERP therapist can be one of the largest challenges when seeking treatment for OCD," Dr. Eller says. Others may find the process too time-consuming or unaffordable.
For people with treatment-resistant OCD, significant symptoms can persist even after treatment. In such cases, clinicians may recommend trying other options or augmenting ERP with another treatment approach.
Healing happens through strong relationships
Compassionate, experienced mental health professionals focused on evidence-based care


.png)

Medications
Selective serotonin reuptake inhibitors (SSRIs) and some other medications are also first-line options for treating OCD. They are also often a more accessible first step when ERP therapy isn’t accessible or feasible, says Dr. Eller.
Medications may be prescribed when symptoms are severe or when a person has not had enough of a response from OCD therapy. Medications that may be prescribed to treat OCD include:
- FDA-approved SSRIs: Prozac (fluoxetine), Paxil (paroxetine), Luvox (fluvoxamine), and Zoloft (sertraline), which are FDA-approved for OCD.
- FDA-approved tricyclic antidepressant (TCA) medication: Anafranil (clomipramine), a tricyclic antidepressant, has also been shown to be effective and is FDA-approved for OCD.
- Off-label SSRIs: Celexa (citalopram) and Lexapro (escitalopram) are not specifically FDA-approved for OCD, but they have shown effectiveness in research and are sometimes prescribed off-label.
OCD symptoms can make engaging in ERP feel impossible, Dr. Eller notes. That's when medications can be particularly helpful. "Medications can help decrease the intensity of the OCD thought-behavior cycles," she says.
These medications don't stop intrusive thoughts, but they can help with symptoms of anxiety and improve mood. They’re a helpful option for many people, with up to 60% of patients showing positive results from SSRI therapy.
That said, some people have side effects they can't tolerate or don't get the response they need. In such cases, clinicians may switch to a different type of medication, add ERP as an additional treatment, or consider an adjunctive treatment.
Combining ERP and medications
Many people find that a combined approach that involves both ERP and medication is the most effective option. Medication can make some symptoms feel less intense, which can then make it easier to engage in ERP therapy. ERP helps give people the long-term skills they need to better manage OCD symptoms.
This approach is sometimes particularly helpful for people who have co-occurring mental health conditions such as anxiety or depression. For many, taking a two-pronged approach that includes therapy and medication is often the most effective.
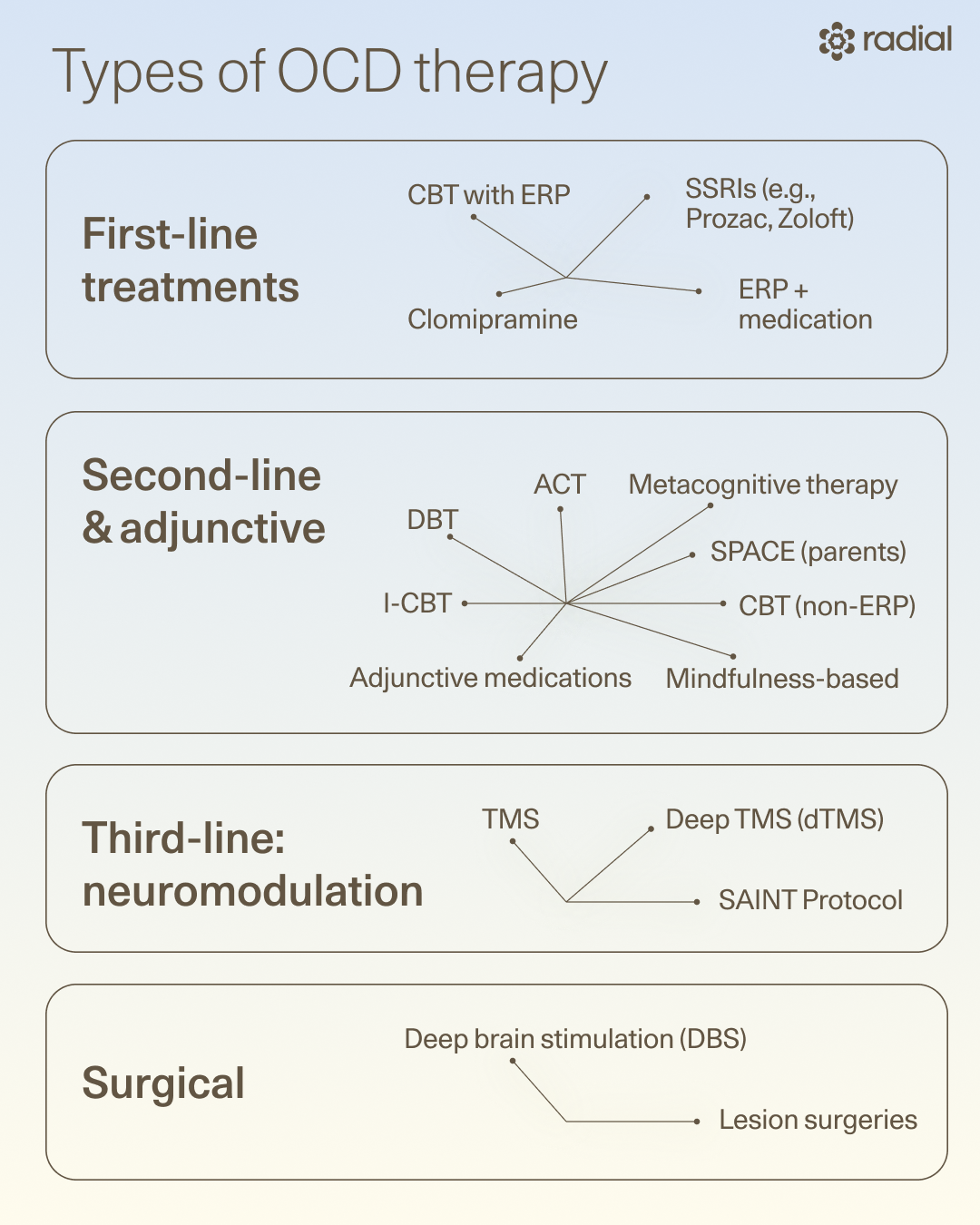
Second-line and adjunctive OCD treatments
While first-line options work well, somewhere between 40% and 60% of people are still left with troublesome symptoms after taking SSRIs, and fewer than half achieve full remission from ERP therapy.
"While ERP and medication (alone or together) can help some people, these options aren't always enough to allow people to go to work and school, or to engage in relationships in a meaningful way," Dr. Eller says.
So what happens if you’ve tried the first-line options but still haven’t gotten the results you’d hoped for? When this happens, clinicians may recommend second-line or adjunctive approaches. Some can be helpful on their own, but they are most effective when paired with ERP, medication, or both.
Cognitive-behavioral therapy (CBT)
Cognitive-behavioral therapy (CBT) can be an effective way to help people with OCD learn to recognize and challenge the distorted thoughts that fuel obsessions. Cognitive distortions like an inflated sense of responsibility (“If I don’t check the oven one more time, the house will burn down and it will be all my fault!”) and overestimating the likelihood of harm (“If I make a mistake at work, it will ruin everything and I’ll get fired and then lose my house!”).
A CBT-trained therapist will guide people through behavioral experiments to gently encourage them to face their fears or thoughts without resorting to rituals or compulsions. It’s a method that helps people see whether their fears are realistic and, over time, gradually reduce the anxiety that fuels OCD. CBT is often used alongside medication to support the skills people are developing to manage their symptoms.
Acceptance and Commitment Therapy (ACT)
ACT is a variation of CBT that helps reduce the anxiety caused by obsessions by changing how people relate to their intrusive thoughts. Rather than trying to control them, this approach teaches people to accept uncomfortable thoughts while focusing on their goals and values. It is often used alongside ERP to help people tolerate uncertainty and reduce avoidance.
Inference-based cognitive-behavioral therapy (I-CBT)
Inference-based cognitive therapy, or I-CBT, targets the feelings of self-doubt that cause people to distrust their own perceptions and behaviors. It focuses on the "what-if" thoughts that drive obsessions and compulsions. Instead of automatically reacting to a worry, this approach teaches people to question their initial assumptions. The goal is to help people distinguish between a realistic thought and an irrational one, which can help disrupt the OCD cycle.
For example, a thought like "What if I forgot to lock the door and someone breaks in" turns an ordinary, everyday situation into a high-stakes threat. It teaches people to tolerate uncertainty more effectively and helps them trust themselves more. It can be used alongside ERP or as a stand-alone treatment for OCD.
Metacognitive Therapy
OCD isn’t just shaped by intrusive thoughts, but also by what people believe these thoughts mean. Metacognitive therapy focuses on these beliefs, a process often called metacognition. It helps people relate to their thoughts differently, instead of getting caught up in what they think they might mean.
People with OCD sometimes see a thought as dangerous or harmful in and of itself. For example, they might mistakenly think, "Having this thought means something bad might happen" or "If I don't do something to get rid of this thought, I might act on it."
Metacognitive therapy can help minimize those beliefs and reduce the need to engage in compulsive behaviors. It’s usually combined with treatments, and research suggests it can be helpful for people who haven't had enough success with ERP therapy.
Second-line and adjunctive medications
When first-line medications are not sufficiently effective, clinicians may adjust doses, switch medications, or add other medicines, such as antipsychotics. These may include:
- Risperdal (risperidone) and Seroquel (quetiapine), which are second-generation antipsychotics, are two examples.
- Serotonin-norepinephrine reuptake inhibitor (SNRI) medications such as Effexor (venlafaxine) or Cymbalta (duloxetine) may sometimes be prescribed, although there is not as much evidence to support their effectiveness in the treatment of OCD.
In most cases, these medications are used alongside other proven treatments, such as ERP and SSRIs, rather than on their own.
Supportive parenting for anxious childhood emotions (SPACE)
SPACE is a treatment for OCD designed for the parents and caregivers of kids with the condition. It teaches parents to respond in ways that support OCD recovery rather than unintentionally reinforcing symptoms. For example, parents may do things like provide reassurance, change routines, or participate in rituals that, while easing a child's distress, keep the OCD cycle going.
By learning new ways to respond, parents help their child gradually reduce OCD symptoms. One beneficial aspect of SPACE is that it doesn't require the child to attend therapy sessions. This can be helpful for kids who are overwhelmed or resistant to treatment.
Dialectical behavior therapy (DBT)
Originally developed to treat borderline personality disorder, DBT is also used for other conditions to help people tolerate distress and manage emotions. DBT for OCD is not usually a primary treatment, but it can be useful for augmenting ERP since it may improve emotion regulation and distress tolerance skills. That can help when intense emotions make OCD treatment feel challenging. Teaching people to better tolerate feelings of anxiety makes them less likely to engage in compulsions.
Mindfulness-based therapy
Mindfulness-based approaches can help people notice intrusive thoughts as they happen without automatically reacting to them. The first thing people with OCD often do when they have an intrusive thought is to try to suppress it or neutralize it by engaging in compulsive behavior. Mindfulness teaches people to observe their thoughts with less judgment and tolerate them with less distress.
This approach doesn’t focus on eliminating intrusive thoughts. Instead, it works by reducing the urge to engage with them. The result is that it often becomes easier to sit with feelings of anxiety while resisting compulsions. These techniques are often used to complement ERP rather than replace it.
Third-line OCD treatments
Third-line treatment options for OCD are sometimes considered when OCD is severe, relapsing, or has not responded well to first- and second-line options. Such options are often more intensive and specialized.
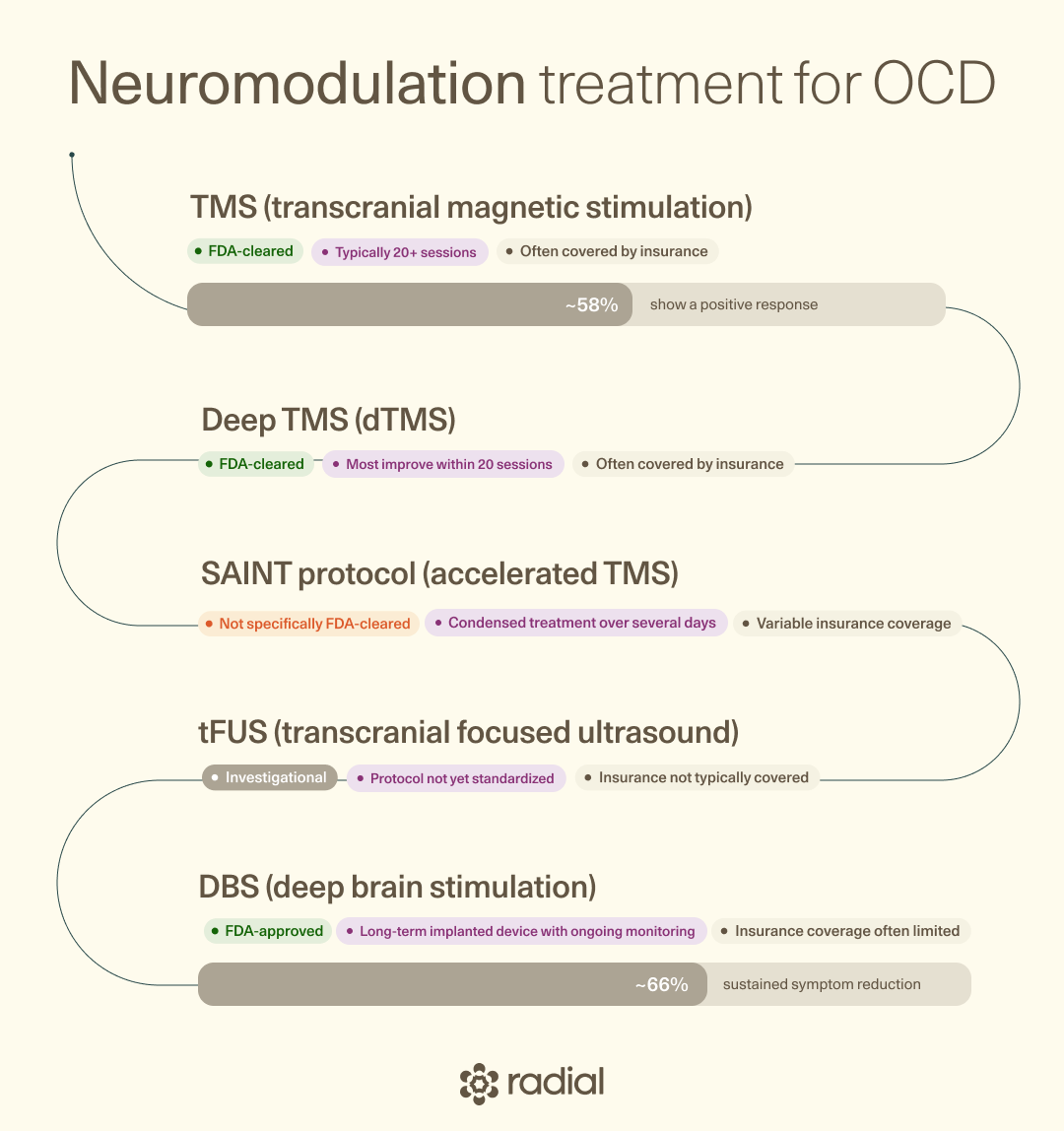
Transcranial magnetic stimulation (TMS)
Neuromodulation can be the next best step if ERP and medication haven't helped enough, Dr. Eller says. Transcranial magnetic stimulation (TMS) utilizes electromagnetic pulses to target specific areas of the brain that play a role in OCD symptoms. "It can specifically target parts of the OCD brain circuit leading to significant symptom relief," she explains.
This approach is FDA-cleared for treatment-resistant OCD and is used when ERP and medications have not produced sufficient results. "If you have tried two or more medications without relief, your OCD is considered ‘treatment-resistant’ and would be a good candidate for TMS," says Dr. Eller.
It can also be a highly effective and cost-efficient OCD treatment, with 58% of people experiencing a positive response to treatment. It’s also been shown to be safe, with limited side effects like mild headache or scalp irritation. Radial offers both traditional and advanced TMS options, including SAINT, BrainsWay, and AMPA.
Deep TMS (dTMS) and SAINT
Deep TMS targets deeper brain areas than standard TMS. It is specifically cleared to treat OCD. For OCD, dTMS often uses the H7 coil targeting a distinct area of the brain associated with OCD. This same coil has shown effectiveness for major depressive disorder, which can be helpful when there are co-occurring mood symptoms that overlap with those observed in OCD.
SAINT is a newer, accelerated TMS protocol that can produce rapid results.
Real-world research has shown that most people treated with dTMS show improvements in OCD symptoms within 20 sessions. Longer treatment sessions were also linked to better results, suggesting that extended treatments might be a helpful option for people who have treatment-resistant OCD.
Deep brain stimulation (DBS)
DBS is a surgical option that involves implanting electrodes in targeted areas of the brain. Mild electrical pulses then help modulate the brain activity that is linked to OCD symptoms.
It is FDA-approved for OCD, but it’s typically considered only when symptoms are severe, chronic, and treatment-resistant, since it is invasive and does pose some neurological risks. Its use is also often limited simply because many insurance providers do not cover the costs as a treatment for OCD.
Dr. Eller says this option can provide relief for the most severe cases where nothing else has worked. It can be a lasting, effective option for some people, with around two-thirds of patients showing sustained symptom reduction.
Surgery
Surgical options, such as anterior cingulotomy and anterior capsulotomy, involve operating on specific areas of the brain to reduce OCD symptoms. These procedures create small lesions on key brain areas to disrupt the circuits involved in OCD symptoms. Such surgeries are usually only considered in severe cases where a person has not responded to other treatments.
Emerging and experimental OCD treatments
Other options are also still being explored and are sometimes used selectively to treat OCD. While many of these show early promise, they are not yet considered standard care when it comes to relieving symptoms of OCD. In other words, they are best seen as add-ons or experimental options rather than as primary treatments.
Transcranial focused ultrasound (tFUS)
Transcranial focused ultrasound (tFUS) is an emerging treatment for OCD that utilizes non-invasive neuromodulation using low-intensity sound waves. Research suggests that it has potential as a later treatment for OCD in situations where other treatments have been ineffective. It works by modulating deeper brain regions, such as the ventral capsule/ventral striatum (VC/VS), and may be a safer alternative to deep brain stimulation.
Psychedelics
Psilocybin has been one of the buzziest mental health treatment options in recent years, including in the treatment of OCD. One small study found that a single dose of psilocybin led to significant reductions in symptoms for up to a week. Longer courses of treatment may produce better results, but this needs further research. Exactly how it works to improve OCD symptoms also isn’t fully understood.
Ketamine
Studies suggest that ketamine therapy has promise as a fast-acting option for treatment-resistant OCD. It works by modulating glutamate in the brain to help rewire the brain pathways involved in OCD. It can also help target the OCD cycle itself, ‘loosening’ the connection between thoughts and behaviors, which can make it easier to break out of those rigid, distressing patterns.
While not FDA-approved, research on ketamine for OCD has shown promise. Patients who took a single dose reported fewer intrusive thoughts and compulsions, often working within a week, which can make it an appealing option for people who haven’t had much luck with other options. However, some people have found that these results may wear off somewhat quickly, which is why it might be best used when combined with ERP or other therapies.
Supplements
It’s no secret that nutrition can play a role in mental health, which is why researchers are also exploring how certain supplements might have a supportive role in treating and managing OCD symptoms. Options that may help support brain health and influence how brain cells communicate include:
- N-acetylcysteine (NAC): An antioxidant that may help reduce glutamate levels in the brain. Dysregulation in this brain chemical may contribute to OCD symptoms. While more research is needed, some studies have shown that NAC supplementation can lead to significant reductions in Y-BOCS scores.
- 5-HTP: 5-hydroxytryptophan is a compound that the body can convert to serotonin and melatonin, which is why it has been explored as a potential treatment for conditions like depression, insomnia, and OCD. Evidence suggests that it might be helpful as an add-on treatment for moderate and severe OCD, but more research is needed.
- B12: This vitamin influences the brain chemicals involved in mood regulation, and having low B12 levels has been connected to worse OCD symptoms. Taking this supplement (or eating foods rich in B12) won't treat OCD on its own, but it's a good idea to talk to your doctor about testing your B12 levels if you are concerned.
Other supplements that have been explored for their potential to manage OCD symptoms include glycine, myoinositol, milk thistle, valerian root, folic acid, and vitamin D. Just how effective these options might be, however, is still unclear and needs further research.
For now, supplements are best used as a way to augment–not replace–other treatments like therapy and medication. Because supplements can interact with medications or affect existing health conditions, it’s always important to talk to your doctor first before you make the decision to try them.
Pharmacogenomic (PGx) testing
Finding the right medication to treat OCD sometimes takes a few tries to get right–so what if there was a way to ease that process and inform treatment options a little quicker? That’s the goal of PGx testing, which looks at how your genes might affect the way your body responds to certain medications.
It’s usually done by taking a cheek swab and analyzing specific genes. This can give clinicians extra insight into how you might respond to different antidepressants, including which might help and which are more likely to cause side effects.
It’s not foolproof and can’t predict exactly how each person will respond, but PGx testing may cut down on some of the trial and error when it comes to finding the right OCD medication and dose.
Lifestyle changes that help with OCD
OCT treatment doesn't take place in a vacuum. Everyday habits, like how you sleep, eat, and care for yourself, all affect how you feel and how you engage with recovery. While lifestyle changes aren’t a treatment for OCD on their own, they can make a big difference in how you feel day to day.
Supportive changes can help you feel your best
- Sleep: Getting enough consistent sleep can help with emotional regulation and lower overall anxiety, which may make obsessive thoughts less intense and overwhelming.
- Exercise: Staying physically active can help improve mood and lower anxiety, which may also make intrusive thoughts more manageable.
- Diet: Eating a balanced diet can help support energy levels and brain health. Diet won't cure OCD, but eating a balanced diet can improve mood regulation and reduce stress reactivity.
- Stress management: Stress can make OCD symptoms worse. Utilizing breathing exercises and other relaxation techniques can help keep stress and anxiety in check.
- Routine and structure: Establishing predictable daily routines can help you feel more in control and stable. When your day feels more certain, you're less likely to be overwhelmed with anxious thoughts or compulsive urges.
- Avoiding substances: It’s also important to limit alcohol, caffeine, and recreational drugs. People with OCD may have an elevated risk of substance use problems, which can complicate treatment and make it harder to manage symptoms.
- Social support: Supportive relationships can help people feel connected and less isolated. Feeling supported by people in your life may even help lessen the severity of some OCD symptoms.
Relief within reach
Care covered by your insurance
Radial provides advanced mental health treatment, covered by the insurance you already use.








OCD treatments to avoid
In addition to understanding which treatment options are the most effective and supported by evidence, it’s helpful to know which ones to avoid. Treatments that are sometimes marketed for OCD lack sufficient evidence or waste time that would have been better spent on more effective options. These approaches are not recommended as primary treatments:
- Eye Movement Desensitization and Reprocessing (EMDR): EMDR is a type of therapy that uses bilateral eye stimulation to help people process traumatic memories. While well-supported in the treatment of PTSD, its use for the treatment of OCD hasn’t been established.
- Hypnotherapy: There is no evidence for treating OCD.
- Thought field therapy (TFT): Lacks scientific support and is considered pseudoscientific.
- Brainspotting: This is a type of body-focused therapy that uses eye positions to process difficult emotions and memories. It has limited evidence and no clear mechanism for OCD treatment.
- Herbal remedies: Not supported by evidence and may interfere with medications
- Acupuncture: No convincing evidence that it improves OCD symptoms
- Biofeedback: Some limited research has shown it may be helpful, but it has not been sufficiently studied as an OCD treatment
- Chiropractic treatment: No evidence for OCD; unrelated to the disorder's mechanisms
Certain medications may sometimes be used off-label, but they are not recommended as stand-alone OCD treatments. They should only be prescribed by clinicians with OCD expertise. These medications include:
- Benzodiazepines: Can help reduce anxiety in the short-term, but carry a risk for dependence, so they are generally not recommended.
- Lithium and anticonvulsants: While there have been some small studies looking at their use, lithium and anticonvulsants are not supported as treatments for OCD.
Where to start: A practical action plan
The many options for treating OCD can be a lot to take in, especially when you're dealing with symptoms right now. What's important to remember is that you don't have to do it all at once. Getting started is the most important step, and you can work with your clinician to move forward one step at a time. Here’s a clear plan of action to help guide your OCD journey:
- Get a clear diagnosis. If you haven't already, talk to a clinician who understands OCD and has experience treating it. They can use tools like the Y-BOCS to evaluate symptoms, confirm your diagnosis, assess severity, and track your progress throughout treatment.
- Find an ERP-trained provider. Specialized treatment is crucial when it comes to OCD interventions. Look for a therapist who has training and experience specifically with exposure and response prevention.
- Start an evidence-based treatment. For most people, this means beginning ERP and sometimes taking medication depending on their symptoms. It's normal for progress to take time, and you may experience some discomfort as you face your fears and adjust to your medications.
- Adjust or combine treatments as needed. If you find that the first-line approach to treatment hasn't improved your symptoms enough, adding an adjunctive option like ACT, cognitive-behavioral therapy, or medication adjustments might help support your progress.
- Reassess and consider second-line options. After you've tried first-line treatments fully and haven't seen sufficient benefits, second-line therapies or medications may be an appropriate option.
- Continue advocating for your care and consider third-line options. Many people find that first- and second-line options work well, but some people may still have ongoing symptoms, particularly those with treatment-resistant OCD. At this point, it's reasonable to ask about your next steps and to start considering other specialized options. A lack of improvement means that your plan needs to change, not that recovery is out of reach.
If you're ready to take the next step, schedule a consultation with a Radial provider who can help you find the OCD treatment plan that works for you.
The bottom line
OCD symptoms can feel distressing and overwhelming, but effective care can break the OCD cycle of obsessions and compulsions. Exposure and response prevention (ERP) therapy is usually the first step, sometimes in combination with medication. When that doesn't provide the results you need, additional supports, including second-, third-, adjunctive-, and experimental options, are also available.
OCD treatment is about figuring out what works for you. If the first approach doesn't work, it means you need to keep working with your clinician to find the right approach and combination of supports. Meaningful improvement is within reach, so you can regain control of your life and get back to your normal routines. If you’re ready to take the next step, Radial can help you develop a personalized treatment plan and explore the options that might work best for you.
Key takeaways
- First-line treatment for OCD usually starts with ERP, which targets the OCD cycle. Medication may also be used to help improve symptoms.
- Second-line and adjunctive treatments can also be helpful when first-line options aren't sufficient or are poorly tolerated, and third-line treatments like TMS and DBS are also options, particularly if OCD has been shown to be treatment-resistant.
- Emerging and experimental treatments might be an option when OCD symptoms are severe or don’t respond to other methods.
- If you're ready to start, getting a clear diagnosis, finding a therapist trained in ERP therapy, and starting treatment are the first steps. From there, you can work with your clinician to monitor your progress, adjust or add on other tools, and move on to third-line options like TMS if medication and therapy don't provide the results you need.
Frequently asked questions
What is the best treatment for OCD?
Exposure and response prevention (ERP) therapy is considered the go-to treatment for OCD, but that doesn't mean that it's the best choice for everyone. Around 60% of people see positive results, but some people have persistent symptoms and need additional support. Other options like cognitive therapy, TMS, and medications can also be helpful. "It's important to remember that the best treatment for OCD is usually a combination of treatments," Dr. Eller says. For many, this may include therapy, medications, and another option like TMS.
Why is OCD so hard to live with?
The OCD cycle creates a cycle of thoughts and compulsions that are distressing and time-consuming. It makes it hard to function in daily life and leads to feelings of anxiety, exhaustion, and stress that can be incredibly overwhelming. People with the condition experience a lot of shame about their symptoms. "They know their intrusive thoughts and the behaviors that follow 'don't make sense.’ Because of this, the symptoms of OCD can go undiagnosed for years," Dr. Eller says. That can lead some people to feel like finding relief is out of reach. While it can be hard to live with, effective treatments can help you get control of this cycle so you can get back to living your life.
Can I ever live a normal life with OCD?
Yes, you can absolutely live a normal life with OCD. Managing the condition requires seeking effective treatments, such as ERP and medication, to help you control your symptoms.
Can OCD be cured?
OCD is a chronic condition, and relapses can happen, so it can't necessarily be "cured" in the traditional sense. However, specialized treatments have high effectiveness rates and can help people significantly improve their symptoms. Instead of thinking of it as a cure, think of it as a way to manage it, much like managing other chronic illnesses like asthma, diabetes, and migraines.
Deep dive recommendations
- David Puder, MD, Psychiatry & Psychotherapy Podcast. Episode 228: Comprehensive obsessive-compulsive disorder (OCD) treatment guide: Evidence-based ERP approaches and best practices for clinicians.
- National Institute on Mental Illness (NIDA). My life with OCD.
Editorial Standards
At Radial, we believe better health starts with trusted information. Our mission is to empower readers with accurate, accessible, and compassionate content rooted in evidence-based research and reviewed by qualified medical professionals. We’re committed to ensuring the quality and trustworthiness of our content and editorial process–and providing information that is up-to-date, accurate, and relies on evidence-based research and peer-reviewed journals. Learn more about our editorial process.
Let's connect
Get started with finding the right treatment for you or someone you care about
Get startedExplore more posts