TMS for OCD Treatment: Is It Effective and Who Is It For?
If you’ve tried therapy and medication for OCD and still feel stuck, you’re not alone—and you’re not out of options. TMS is a research-backed approach that targets the brain circuit involved in OCD. It’s often used when other treatments haven’t worked well. And for many people, it can create a meaningful shift, making symptoms feel more manageable and other therapies more effective.
If you’re here, you’ve likely put in a lot of work to manage OCD. Maybe you’ve done exposure and response prevention therapy. Maybe you’ve tried one or more medications. And maybe, despite all of that effort, things still feel hard. That can be frustrating, exhausting, and discouraging, but you’re not out of options. Enter TMS for OCD.
TMS is a type of non-invasive brain stimulation that’s been cleared by the FDA to treat people with OCD who haven’t gotten enough relief from therapy or medication. In fact, in 2018, BrainsWay’s Deep TMS system became the first-ever non-invasive medical device granted De Novo clearance to treat the condition. It targets specific brain circuits involved in OCD, with the goal of helping those patterns become less intense and easier to interrupt.
Below, we’ll walk through TMS and OCD, including how it works, how effective it is, and what the experience is actually like so you can decide whether it’s a next step worth exploring.
What is TMS and how does it work for OCD?
TMS is an FDA-cleared, non-invasive treatment that uses magnetic pulses to target and regulate brain circuits involved in OCD.
“TMS involves a strong magnetic pulse applied to the scalp, and those magnetic pulses create electrical fields that directly stimulate neurons in the brain,” explains Steve Harvey, MD, FCTMSS, a board-certified psychiatrist and Midwest regional medical director at Radial.
The goal is to interrupt a specific loop in the brain. OCD has many subtypes that all follow a pattern: A thought triggers anxiety, which leads to a compulsion, which briefly relieves that anxiety before the cycle starts again. This creates a frustrating cycle of intrusive,unwanted, and often distressing thoughts, and people seek behaviors to reassure them that the unwanted thought isn't true.
Often, the behavior we engage in doesn't seem at all related to the anxious/unwanted thought, making many people feel like they're crazy for doing it—but overwhelmed by anxiety if they don't. The behaviors that bring relief can be so unrelated to the unwanted thought, and so time consuming, that OCD can often be mistaken for a psychotic disorder.
TMS (sometimes also called deep TMS for OCD) targets brain regions involved in that cycle to help reduce the overactivity that keeps it going, according to Harvey.
Connect with our Clinicians
.png)


What makes TMS for OCD different from TMS for depression?
TMS is still a relatively new treatment for OCD—it received FDA clearance in 2018. But the technology itself has been around much longer: TMS was first FDA-cleared for treatment-resistant depression in 2008. So while it may feel like a new option to people exploring OCD treatment, there’s actually a substantial amount of safety data and clinical experience behind it.
That said, while the core technology is the same, the way it’s used differs.
One key difference is where the treatment is targeted within the brain. TMS for OCD focuses on deeper, midline regions tied to compulsive thinking and behavior (including the dorsomedial prefrontal cortex and anterior cingulate), says Harvey. TMS for depression has traditionally targeted the dorsolateral prefrontal cortex on the side of the brain, though newer protocols may also target the dorsomedial prefrontal cortext.
The goal is also different. Depression-focused TMS aims to improve mood. For OCD, it’s about reducing the intensity and persistence of obsessive thoughts and compulsive urges.
Another key distinction is how it’s used. TMS for OCD is FDA-cleared as an adjunctive treatment (meaning it’s used alongside other approaches). For depression, TMS is FDA-cleared as a standalone option, says Harvey.
Outcomes can vary, too. “The success rates of TMS for OCD are not as good as TMS for depression,” says Harvey. “But in spite of that, TMS is often a great choice for the treatment of OCD after the usual options haven't worked.”
So while it’s not usually a first-line treatment, it can be a meaningful next step when other approaches haven’t been enough.
When is TMS used for OCD?
TMS is typically used to treat OCD when first-line treatments—like exposure and response prevention therapy (E/RP) or medication—haven’t provided enough relief.
For many people, E/RP and medications (like SSRIs) are effective for decreasing symptom severity, which is why they’re still the recommended starting point. But not everyone responds fully. And some people experience unpleasant side effects or symptoms that continue to interfere with daily life.
That’s often where TMS comes in: as a next-step option that targets the brain circuits behind OCD, rather than just the symptoms.
If you reach this point, know that it’s common to try therapy or medication and still feel like something isn’t fully clicking. Exploring additional options doesn’t mean there’s no hope—it just means your brain may need a different approach.
Why TMS is often combined with E/RP therapy
TMS is often used alongside E/RP therapy rather than replacing it—and there’s a reason for that.
Think of OCD as an overactive fire alarm system in your brain: An intrusive thought sets off the alarm, and compulsions are the water your brain releases to put out the fire. Treatments like TMS work on the brain level to help make that alarm system less reactive, while E/RP decreases the flood of water triggered by the alarm.
Put simply, they can complement each other. TMS can make symptoms feel more manageable, while E/RP helps you build new patterns and responses during that window of change.
Some TMS protocols for OCD even incorporate elements of exposure during treatment. “We think [treatment] works better if we provoke the patient's symptoms during the TMS session. If they have obsessive worries about germs, for example, then we might have them rub the carpet with their hand right before treatment,” explains Harvey. “The goal is to activate their OCD symptoms, but not so much that we cause extreme distress.”
That might sound counterintuitive at first, but it's done in a controlled, collaborative way. The idea is to activate the specific brain circuits involved in OCD so the stimulation can target them more directly, he says.
It’s also worth noting that some people hope TMS will replace therapy altogether. But in most cases, results are the strongest when it’s part of a broader treatment plan. The goal of treatment is to give people back a sense of control. No treatment is curative; maintaining improvement often means a long-term practice of incorporating exposure and response prevention (ERP) skills and supportive healthy brain circuits with medications and/or TMS.
How effective is TMS for OCD?
ERP therapy tends to have the strongest long-term results for OCD. And medications like SSRIs can also reduce symptoms for 40-60% of people (though many continue to experience symptoms that affect daily life).
But OCD treatment isn’t one-size-fits-all, and some people still feel stuck even after putting real effort into those approaches. And while TMS effectiveness rates for OCD aren’t as high as they are for depression, Harvey says it can still be a worthwhile treatment for people who haven’t gotten enough relief from other options.
In one pivotal clinical trial, about 38% of people responded to TMS after six weeks, rising to about 45% at one-month follow-up. And while most studies measure “response” rather than full remission, meaningful symptom reduction can make day-to-day life feel much more manageable.
Progress is often measured using tools like the Yale-Brown Obsessive Compulsive Scale (Y-BOCS), which tracks symptom severity over time. Rather than expecting symptoms to disappear completely, effective TMS treatment usually means OCD feels less disruptive day to day.
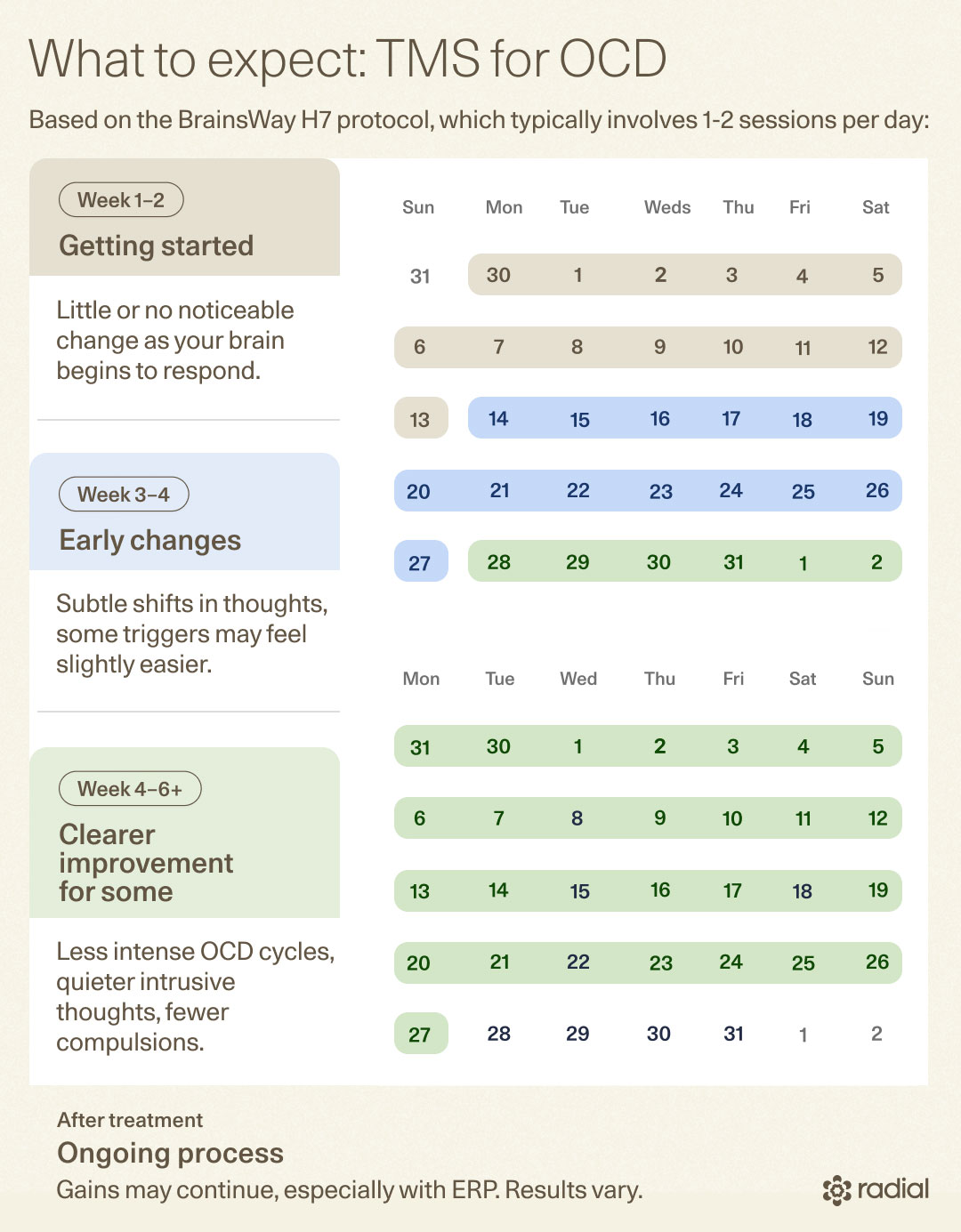
Most people also don’t notice immediate changes. That can feel discouraging at first, but it’s a normal part of the process. TMS works gradually, with subtle shifts often appearing after a few weeks and clearer improvements for some as treatment continues. Progress can even continue beyond the treatment period, especially when paired with E/RP.
Ultimately, not everyone responds the same way. Some people see clear improvement, others notice those gradual shifts, and some may not experience much change. But even small gains can matter, especially if they make it easier to engage in therapies like E/RP.
What is TMS therapy for OCD like?
TMS therapy for OCD is a structured outpatient treatment that happens over multiple sessions. And while the basics are similar to TMS for depression, there are a few key differences.
One of the biggest is something called symptom provocation. In some OCD protocols, you’ll briefly focus on a trigger before or during treatment to activate the brain circuits involved, says Harvey. That way, the stimulation is targeting the right pathways in real time.
While that can sound overwhelming, know that the process is done with support and intention—you’re not pushed beyond what feels manageable.
TMS sessions for OCD follow a consistent process, though timing can vary. Traditional TMS protocols are delivered over several weeks, while accelerated TMS compresses sessions into a shorter timeframe. Your provider will work with you to choose an approach that feels best for your needs.
In general, though, here’s what to expect:
- Getting set up: You’ll sit in a comfortable chair while a provider positions the TMS coil device on your head. No anesthesia or sedation is needed—you’re awake the whole time.
- Symptom activation: You may be asked to briefly think about or engage with a specific OCD trigger to activate the relevant brain circuits.
- Stimulation: The machine delivers a series of magnetic pulses. You won’t feel the brain stimulation itself, but you may notice a tapping sensation on your scalp.
- Session length: Accelerated TMS sessions typically last less than 10 minutes. Traditional TMS sessions can last for up to 45 minutes each.
- Frequency: For accelerated TMS, you’ll receive around 50 TMS sessions over five to 10 days. For traditional TMS, you’ll receive around 36 sessions over four to six weeks.
- After the session: You can return to your normal routine right away—there’s no recovery time needed.
It can sound a little intimidating at first, but in practice, most people find TMS quite manageable. “The stimulation affects the nerves and muscles of the scalp itself, which makes it feel like a tapping on the head,” says Harvey. “Any discomfort from the treatment is usually mild.”
TMS side effects and safety
It’s completely normal to have questions or concerns about TMS side effects. The good news is that TMS for OCD is considered safe and well-tolerated.
Because it doesn’t require anesthesia or affect the whole body, most side effects are mild, limited to the treatment area, and often ease as your body gets used to treatment. You stay awake and alert during each session, and most people return to their normal routine afterward. Unlike some other treatment options, there is no memory impairment and you can drive yourself to and from treatment.
The most common side effects include:
- Scalp discomfort: A tapping or tingling sensation at the treatment site, especially early on, that often improves over time
- Headache: Usually mild and temporary; often resolves on its own or with over-the-counter medication
- Facial twitching: Can happen during stimulation due to nearby nerve activation, but stops once the session ends
More serious side effects are rare, but it’s still important to be aware of them. In very rare cases, TMS has been associated with seizures. There’s also a risk of hearing-related side effects—like tinnitus or changes in hearing—which is why ear protection is typically recommended during treatment. Your provider will carefully screen for any risk factors beforehand to keep you as safe as possible.
Who is a good candidate for TMS for OCD?
TMS for OCD isn’t the right fit for everyone, but it can be a strong option if you haven’t gotten enough relief from standard treatments and are looking for a next step.
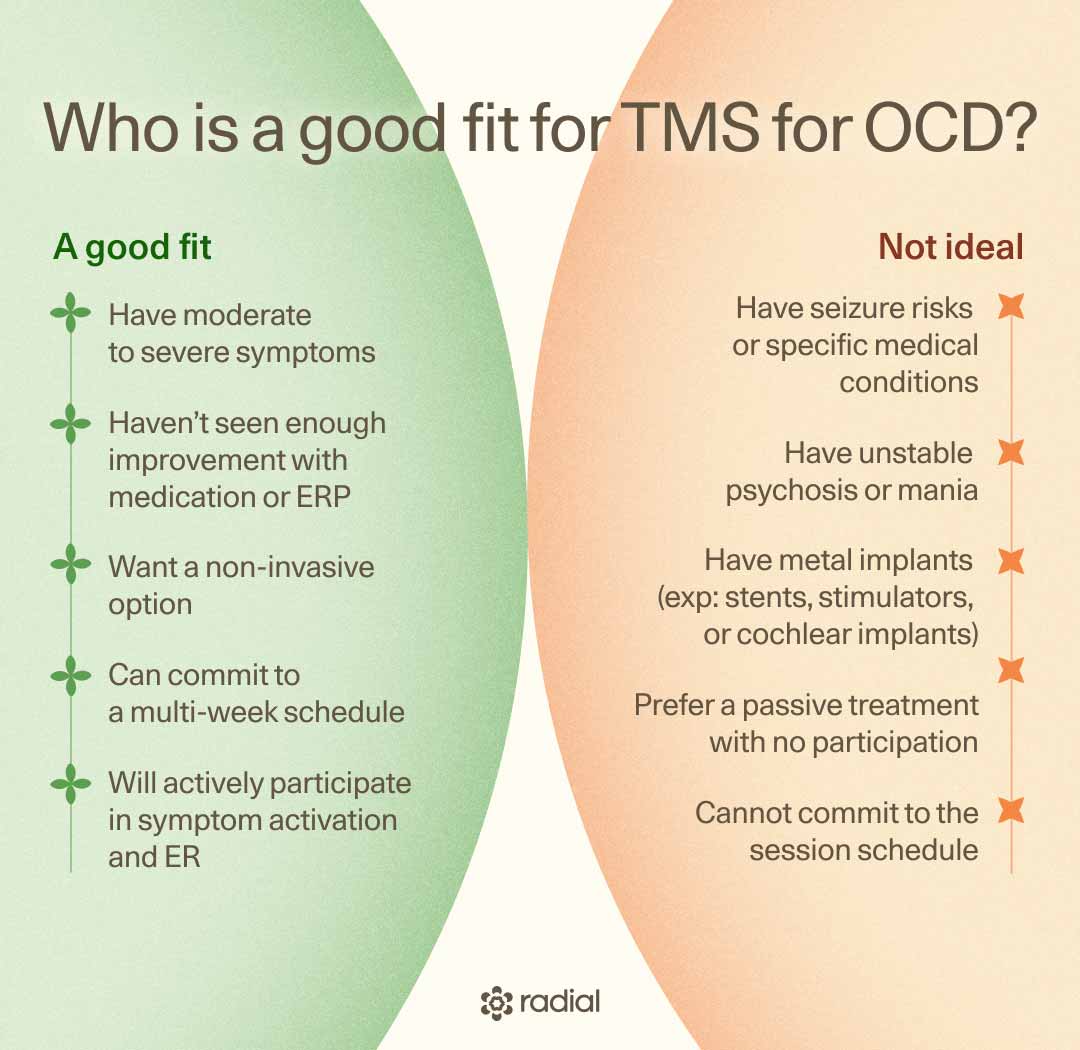
In general, TMS may be a good fit if you:
- Have moderate to severe OCD symptoms
- Haven’t responded enough to ERP therapy, medication, or both
- Are looking for a non-invasive treatment option
- Are able to commit to a structured treatment schedule over several weeks
- Are open to actively participating in treatment (including symptom activation and, often, E/RP)
On the other hand, TMS may not be ideal if you:
- Have certain medical conditions that increase seizure risk
- Have untreated or unstable conditions like active psychosis or mania
- Have metal or implanted medical devices (like stents, deep brain stimulators, or cochlear implants) that may not be compatible with the strong magnetic field used in TMS
- Are expecting a fully passive treatment without any participation
- Are unable to commit to the treatment schedule
That said, none of these lists are definitive. The best way to know if TMS is a good fit is to talk with a provider. They can walk through your history, current symptoms, goals, and insurance coverage to help you weigh whether it makes sense as a next step.
It’s also worth noting that access can be a factor. “Another important thing to remember is that many insurance plans won't cover TMS for OCD,” says Harvey.
If your insurance doesn’t cover treatment, don’t worry—it’s not the end of the line. Some clinics and nonprofits offer financial support or payment plans. You can also use money from your health savings account (HSA) or flexible spending account (FSA) to help cover treatment.
How to decide if TMS is right for you
Deciding whether to try TMS for OCD isn’t always straightforward, especially if you’ve already tried other treatments and are feeling unsure about what to do next. As you explore TMS as an option, the goal is to understand whether it fits your situation and what you’re looking for.
It can help to start by considering a few questions:
- Have I given first-line treatments like E/RP and medication a fair try?
- Are my symptoms still interfering with daily life in a meaningful way?
- Am I open to a structured treatment schedule over several weeks (or a shorter, more intensive version)?
- Am I willing to actively participate in treatment, including engaging with triggers during sessions?
Most importantly, though, you don’t have to figure this out on your own. Talking to a specialist can help you understand how TMS fits alongside other options, walk through the pros and cons, and assess whether you’re a good candidate.

What happens if it doesn’t work?
This is a fair—and important—question. Not every treatment works for everyone, and that includes TMS. But if it doesn’t lead to the results you were hoping for, it doesn’t mean you’re out of options.
In some cases, providers may adjust the approach by changing stimulation intensity or combining TMS more intentionally with therapies like ERP. Even a partial response can help make symptoms more manageable and other treatments easier to engage with.
There are also other paths to consider. “Better TMS might be right around the corner, so that is an option for the future,” says Harvey. “And some patients might consider deep brain stimulation for OCD. That’s an option that is rarely used, but effective.”
In other words, not responding to one treatment doesn’t mean nothing will work. It just means finding the right approach may take time—and that’s a normal part of treating OCD.
Relief within reach
Care covered by your insurance
Radial provides advanced mental health treatment, covered by the insurance you already use.








The bottom line
TMS is a research-backed treatment that targets the brain circuits behind obsessive-compulsive disorder. It’s typically used when first-line options haven’t provided enough relief.
It’s not a quick fix, and it doesn’t work the same way for everyone. But it offers a different approach—one that focuses on shifting the underlying patterns that keep OCD stuck. For many people, that can make symptoms feel more manageable and open the door for other treatments to work more effectively.
If you’re feeling stuck, exploring TMS doesn’t mean you’re starting over. You’re building on the work you’ve already done. And with the right guidance, it can be a worthwhile next step to consider.
Key takeaways
- TMS for OCD is an FDA-cleared, non-invasive treatment that targets the brain circuits involved in obsessive-compulsive disorder.
- It’s typically used after first-line treatments like E/RP therapy and medication haven’t provided enough relief.
- The TMS for OCD success rate is as high as 58%(response rate), though results vary.
- TMS works gradually, with changes often building over several weeks and sometimes continuing after treatment ends.
- It’s often most effective when combined with therapies like E/RP, rather than used on its own.
Frequently asked questions (FAQs)
What is the FDA approval status of TMS for OCD?
TMS is FDA-cleared for treating OCD in adults. It was first approved for treatment-resistant depression, and later cleared for OCD using specific protocols designed to target the brain circuits involved in obsessive-compulsive symptoms.
Is TMS safe for OCD?
TMS is considered safe and well-tolerated. It’s non-invasive, doesn’t require anesthesia, and most side effects are mild (like temporary scalp discomfort or headaches). Serious side effects are rare, and your provider will screen you ahead of time to help ensure safety.
How long does TMS take to work for OCD?
TMS works gradually. Most people don’t notice immediate changes. But may begin to see subtle shifts after a few weeks, with clearer improvements for some as treatment continues.
Deep dive recommendations
- Transcranial Magnetic Stimulation (TMS) for OCD. International OCD Foundation.
- Obsessive-Compulsive Disorder Treatment. BrainsWay.
Editorial Standards
At Radial, we believe better health starts with trusted information. Our mission is to empower readers with accurate, accessible, and compassionate content rooted in evidence-based research and reviewed by qualified medical professionals. We’re committed to ensuring the quality and trustworthiness of our content and editorial process–and providing information that is up-to-date, accurate, and relies on evidence-based research and peer-reviewed journals. Learn more about our editorial process.
Let's connect
Get started with finding the right treatment for you or someone you care about
Get startedExplore more posts