Postpartum OCD: Why New Parents Experience Frightening Intrusive Thoughts

Those terrifying thoughts about your baby you can’t stop replaying? It could be postpartum OCD—a condition marked by relentless intrusive thoughts, compulsive reassurance-seeking, checking behaviors, and intense fear. Postpartum OCD can be debilitating and understanding what’s happening in your brain is the first step toward feeling better. You are not alone, and help is available.
You finally get the baby down for a nap and a terrifying thought hits: What if they stop breathing and don’t wake up? Five minutes later, you’re standing over the crib checking their chest. Then you check again. And again. Maybe you zoom in on the baby monitor when you’re downstairs. Maybe you Google infant sleep safety for the hundredth time. These thoughts will not subside, and you can't let them go. And then comes the panic: What kind of parent thinks this?
After my son was born, I struggled with intrusive thoughts too—especially fears about accidentally dropping him or exposing him to germs. And while unwanted thoughts about infant harm are incredibly common among new parents, they can become postpartum OCD (pp-OCD) when they’re relentless, distressing, hard to dismiss, and start driving compulsive behaviors.
One of the most important things to understand is that these thoughts are ego-dystonic—meaning they feel horrifying precisely because they go against who you are and what you value, says MaryEllen Eller, MD, a board-certified adult psychiatrist. People with postpartum OCD are often terrified by their thoughts, not driven by them.
In this article, we’ll break down what postpartum OCD actually is, why it happens, how it differs from postpartum psychosis, and—most importantly—how treatment and support can help.
Connect with our Clinicians
.webp)
%20(1).webp)

What is postpartum OCD?
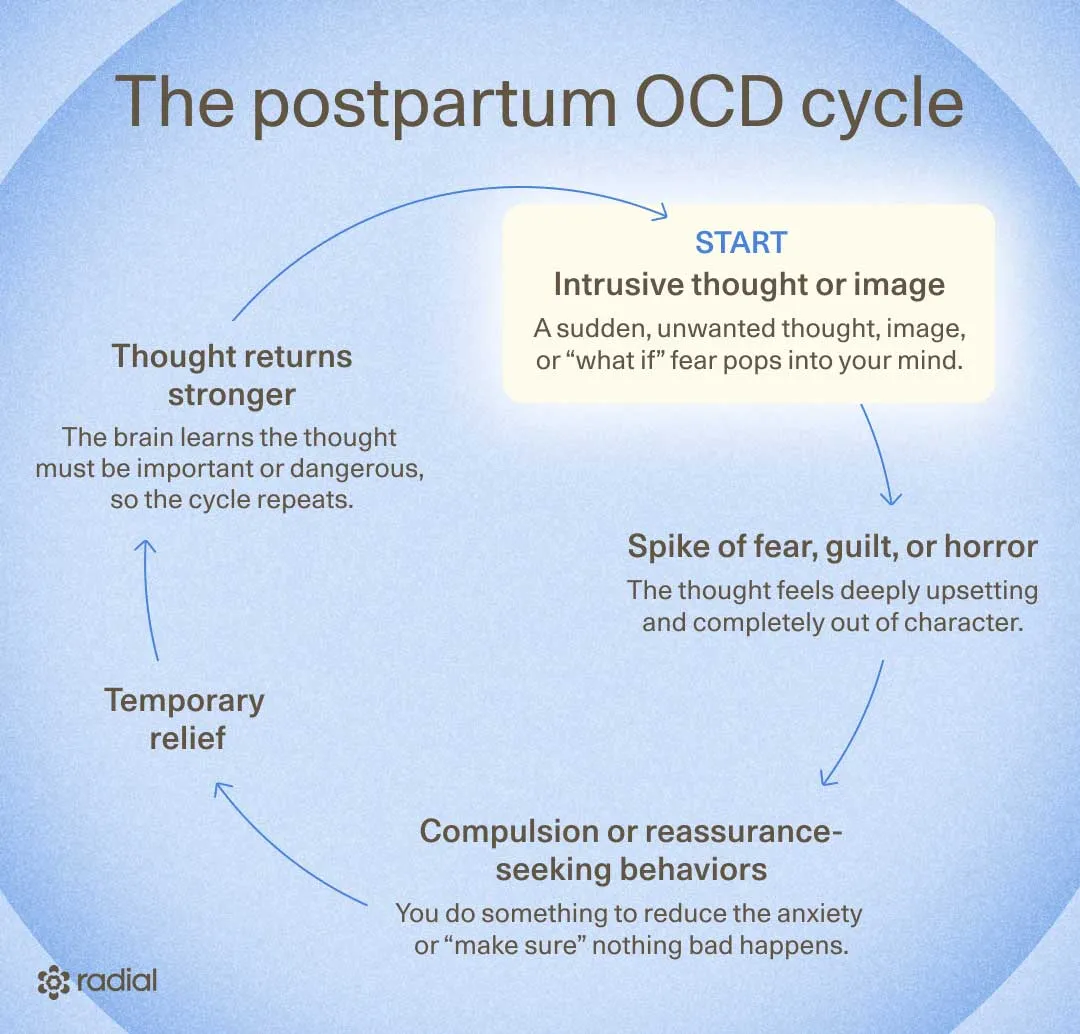
Postpartum OCD is an anxiety-based disorder that can develop after childbirth. Symptom onset can occur in the early postpartum period, with peak prevalence at approximately 8 weeks after delivery. It involves a cycle of:
- Obsessions (thoughts that play on loop, occupy a lot of time, cause a great deal of distress, and significantly impact daily, interpersonal, and executive functioning)
- Compulsions (repetitive behaviors or mental rituals done to ease the anxiety those thoughts create)
The thoughts are upsetting, and people who develop OCD after pregnancy sometimes recognize that their fears or behaviors are excessive, but still feel unable to stop them.
Like other postpartum mental health conditions, postpartum OCD can seriously interfere with daily life and overall well-being. And because the postpartum period comes with huge hormonal shifts, stress, sleep deprivation, and identity changes, it can be an especially vulnerable time for OCD symptoms to appear (or intensify).
What’s the difference between postpartum OCD, postpartum depression and postpartum anxiety?
Obsessions tend to be common in other mental health conditions during the postpartum period, which can make OCD tricky to spot. Anxiety, depression, and OCD can all involve distressing thoughts, rumination, and emotional overwhelm. But there are a few important differences in how they present.
- Postpartum anxiety and depression: Worries are usually tied to real-life concerns (even if they feel excessive), like your baby’s health, sleep, feeding, or your ability to cope.
- Postpartum OCD: Intrusive thoughts feel irrational, disturbing, and repetitive—often centering on senseless fears that don’t shift much over time.
Postpartum OCD vs. postpartum psychosis: An important distinction
Postpartum OCD is often confused with postpartum psychosis because both can involve upsetting thoughts, sometimes about infant harm. But the key difference is insight:
- People with postpartum OCD sometimes recognize the thoughts are irrational, feel horrified by them, and often go out of their way to protect their baby.
- In postpartum psychosis — a rare condition — a person may lose touch with reality through hallucinations, delusions, or severely disorganized thinking, creating potential safety risks for the parent or baby.
Unlike postpartum OCD, postpartum psychosis is a psychiatric emergency and requires immediate medical and psychiatric intervention to reduce the risk of harm. Getting evaluated by a care provider that specializes in perinatal mental health is essential for a proper diagnosis and treatment.
Fear of disclosure: “Will I lose my baby if I tell someone?”
For many parents with perinatal OCD, the scariest part isn’t just the intrusive thoughts—it’s the fear of admitting them out loud. Many worry: What if people think I’m dangerous? What if someone takes my baby away?
That fear is incredibly common, especially when the obsessions involve sexually intrusive thoughts or infant harm. But here’s an important distinction: perinatal healthcare providers should be trained to tell the difference between unwanted intrusive thoughts in OCD and true intent to harm, which can occur in postpartum psychosis.
In OCD, patients recognize the thoughts are unwanted, and their actions “reflect an intense desire to prevent harm,” says Staci Tanouye, MD, FACOG. In other words, being terrified by the thoughts and seeking help for them are actually reassuring signs.
This means: If providers believe both parent and baby are safe, care usually focuses on access to treatment options like therapy, medication, and close follow-up so the parent can start feeling better, says Dr. Tanouye.
The takeaway: postpartum OCD often needs prompt treatment and support, but hospitalization or CPS involvement usually aren’t necessary, she says.
Who gets postpartum OCD?
The postpartum period appears to be a particularly vulnerable time for obsessive-compulsive disorder (OCD) symptoms to emerge or worsen in parents. “The time right after having a baby is one of the riskiest times in a woman's life for OCD to appear,” says Dr. Eller.
Here’s what the research shows:
- Pregnant and postpartum women are about 1.5 to 2 times more likely to experience OCD than the general population.
- Some studies suggest as many as 1 in 6 women experience OCD symptoms during the peripartum period, with other data estimating rates from about 2.43% to 9%
Researchers are still figuring out exactly why postpartum OCD develops, but several factors may increase vulnerability, including:
- being a first-time parent
- a personal history of OCD
- a history of major depressive disorder or postpartum depression
- depressive or anxious symptoms during pregnancy/postpartum
- insomnia or sleep deprivation
- obstetric complications
- certain personality traits, like obsessive-compulsive or avoidant personality styles
What does postpartum OCD actually feel like?
Postpartum OCD is so much more than being “extra worried” or overly careful—it’s a relentless cycle of intrusive thoughts, images, or urges that can cause fear, overwhelming anxiety and self-doubt. These thoughts quietly hijack your mind, consume hours of your day, and make even everyday parenting moments feel terrifying.

Postpartum OCD intrusive thoughts can take many forms
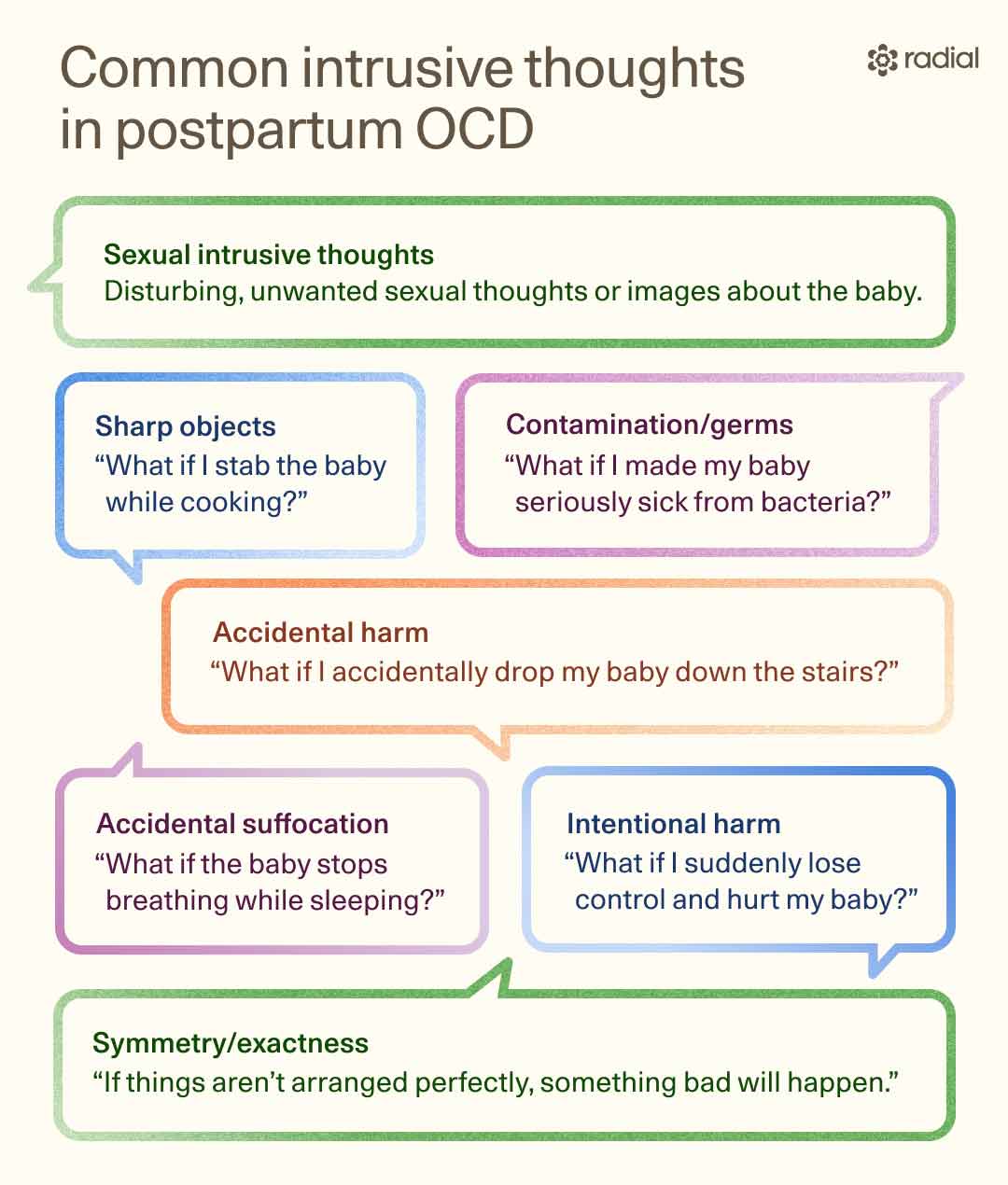
In postpartum OCD, unwanted thoughts tend to center on the baby and usually fall into a few common themes:
- Accidental harm: fears about the baby stopping breathing, suffocating, or dying during sleep
- Intentional harm: disturbing thoughts about dropping, choking, or inappropriate sexual contact with the baby
- Contamination fears: excessive worry about germs, illness, or cleanliness
- Symmetry/exactness: needing things arranged or done in a very specific way
Importantly, intrusive thoughts about infant harm are actually common during the postpartum period even in parents without OCD. It may point to postpartum OCD when the thoughts:
- become persistent, intensely distressing, and hard to dismiss
- start interfering with daily life, bonding, or caregiving
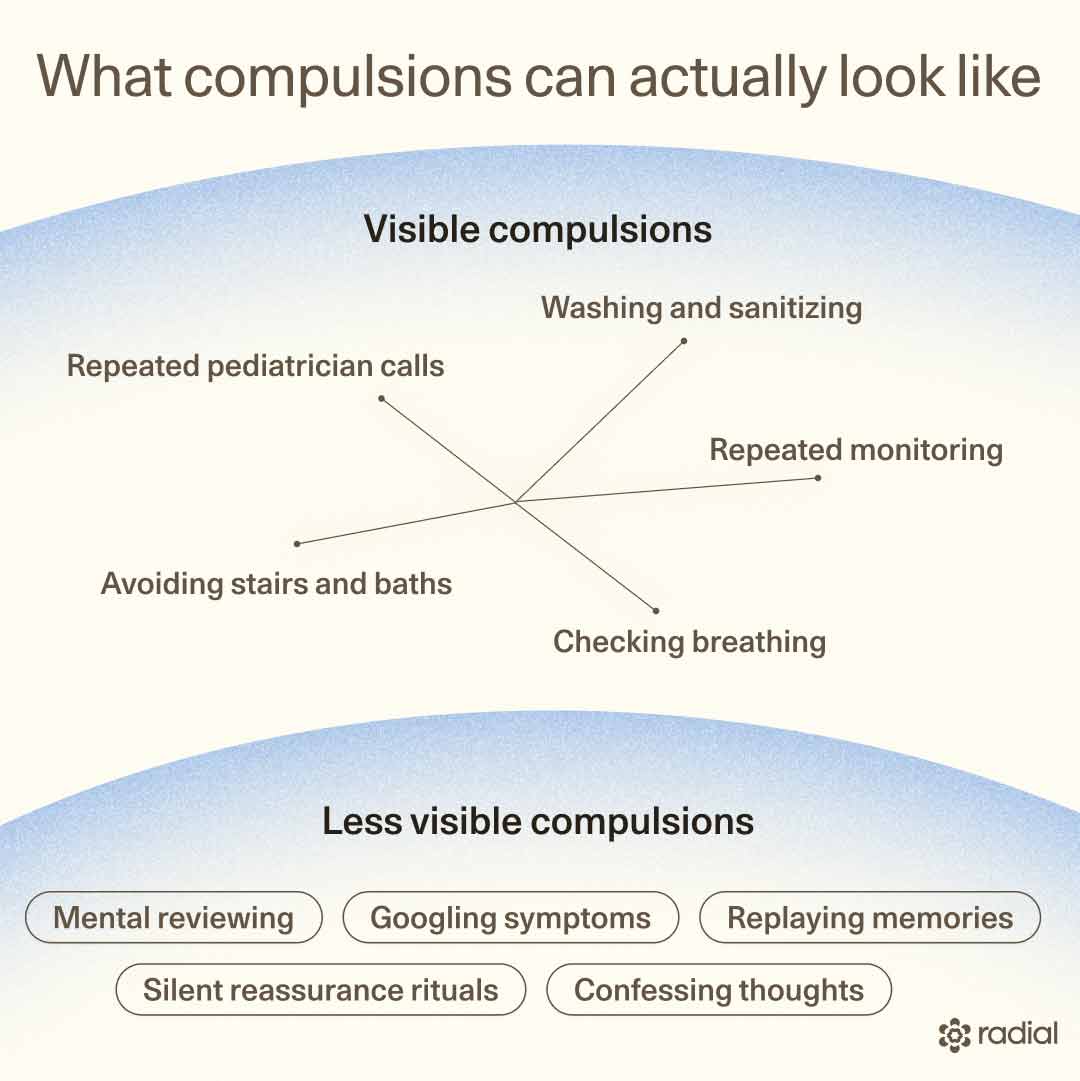
Postpartum OCD compulsions are often less visible
Postpartum OCD isn’t always obvious from the outside. While some compulsions are visible, many happen quietly in a parent’s mind or look like “being extra careful.”
To calm the anxiety triggered by intrusive thoughts, parents may start performing rituals or avoiding certain situations altogether. Common compulsions include:
- Excessive cleaning or sterilizing baby items
- Repeated checking on a sleeping baby
- Constant reassurance-seeking, like Googling symptoms or repeatedly calling the pediatrician
- Avoidance behaviors, such as refusing to bathe the baby, avoiding windows, knives, or certain rooms
- Mental rituals, including praying, counting, or trying to suppress unwanted thoughts
These behaviors may bring short-term relief, but they ultimately keep the OCD cycle going. “Doing rituals like checking, cleaning, praying, or counting brings brief relief, but teaches the brain the wrong lesson: the ritual was necessary and the danger was real,” says Dr. Eller, adding, “Over time the thoughts get stronger and the relief gets shorter.”
In postpartum OCD, most compulsions don’t directly harm the baby. But in severe cases, they can interfere with caregiving—for example, overly aggressive cleaning or extreme avoidance that leads to neglect.
Many parents become afraid of themselves
One of the cruelest parts of postpartum OCD is that parents often become terrified of their own minds. They wonder: What do these thoughts say about me? What if I act on them?
But intrusive thoughts are not intentions. Unlike postpartum psychosis, people with postpartum OCD recognize these thoughts as irrational and unwanted. “The fact that these thoughts horrify you is itself proof that you are not dangerous,” adds Dr. Eller.
Why shame becomes part of the disorder
Postpartum OCD doesn’t just create fear—it often creates crushing shame, too. “Shame and grief often travel alongside postpartum OCD,” says Dr Eller. “Many women grieve the joyful experience they expected and feel deep shame about thoughts that feel unspeakable.”
But here’s the important part: the thoughts feel horrifying precisely because they go against your values. The fear, guilt, and disgust are actually signs that you don’t want to harm your baby. “Having a thought is not the same as wanting it [to happen],” says Dr. Eller, adding, “The distress you feel is actually the proof.”
Unfortunately, stigma makes this even harder. “Mental health is so stigmatized that many feel that any sort of mental health struggle is a personal failure,” says Dr. Tanouye. Add the pressure to seem happy and “okay” postpartum, and many parents stay silent out of fear of judgment.
Shame thrives in secrecy. Staying quiet can delay diagnosis, worsen symptoms, and keep you from getting the support and treatment that can help you feel better.
What causes postpartum OCD?
Experts still don’t fully understand why some parents develop postpartum OCD, but research suggests it’s likely caused by a complicated mix of biological, hormonal, genetic, and environmental factors.
Several mechanisms appear to play a role, including:
- Hormonal shifts: Rapid changes in estrogen and progesterone after childbirth may increase vulnerability to OCD symptoms. Elevated oxytocin levels in late pregnancy and postpartum may influence postpartum OCD symptoms in some people, too.
- Brain chemistry changes: Dysregulation in serotonin, glutamate, and GABA systems may affect mood, anxiety, and obsessive thinking
- Genetics: Certain gene variations linked to OCD and perinatal depression may raise risk
- Stress-response system dysregulation: Overactivity in the body’s stress system (the HPA axis) may contribute
- Neuroinflammation: Inflammation in certain brain circuits may play a role
- Sleep deprivation: Severe sleep disruption—a postpartum classic—can worsen anxiety and obsessive symptoms
- Immune system changes: Immune dysregulation has been linked to both OCD and perinatal mood disorders
- Brain circuit hyperactivity: Increased activity in the cortico-striato-thalamo-cortical (CSTC) circuit appears to be a factor in OCD
How is postpartum OCD diagnosed?
Diagnosing postpartum OCD usually starts with a conversation with your doctor or midwife, who can refer you to a mental health provider. They're “often the first line of help for these patients, and can be critical access points for appropriate diagnosis and start of treatment,” says Dr. Tanouye. That said, if they’re not trained to properly screen for postpartum OCD, they can miss the signs.
“Getting the right diagnosis starts with a thorough evaluation from a licensed mental health provider, and often includes a medical checkup to rule out other conditions that can cause similar symptoms,” says Dr. Eller.
A mental health professional will ask about your symptoms, medical history, family mental health history, and how intrusive thoughts or compulsions are affecting your daily life. Providers may also use screening tools like the Perinatal Obsessive–Compulsive Scale (POCS) or the Parental Thoughts and Behaviors Checklist (PTBC) to better understand the frequency and severity of symptoms.
If you’re struggling and not sure where to start, you can find a licensed specialist using the Postpartum Support International Provider Directory.
How is postpartum OCD treated?
Postpartum OCD treatment is available and getting help can make a huge difference for both you and your family. Experts generally recommend a combination approach that includes therapy, medication, or both.
Exposure and response prevention (ERP) therapy
The first-line treatment for postpartum OCD is a type of therapy called exposure and response prevention (ERP). It’s a specialized form of cognitive behavioral therapy (CBT) with the strongest evidence behind it.
ERP works in two ways:
- Exposure: With the support of an ERP-trained clinician, you gradually face the distressing thoughts, images, or situations that trigger fear.
- Response prevention: You resist the urge to perform the rituals or avoidance behaviors you normally use to reduce anxiety.
Eventually, your brain learns an important lesson: intrusive thoughts are not dangerous, and over time anxiety decreases on its own without compulsions.
Research on postpartum-specific ERP is still limited, but early studies suggest intensive CBT with ERP can be highly effective.
Medication options
Therapy is often the foundation of treatment, but for some people, medication can be an important added layer of support. This is especially true when symptoms are severe, persistent, or making it hard to function day to day.
Research on postpartum OCD medications is still limited, but several medications—FDA-approved for OCD in the general population—are commonly used (and considered safe) during pregnancy and breastfeeding.
First-line options typically include:
- SSRIs (selective serotonin reuptake inhibitors): fluoxetine, fluvoxamine, paroxetine, and sertraline
- Other SSRI options: escitalopram and citalopram may also help, though they are not FDA-approved specifically for OCD
- Clomipramine: a tricyclic antidepressant (TCA)
For severe or treatment-resistant cases, adding an antipsychotic medication alongside an SSRI may sometimes help.
When standard treatments aren't enough
If therapy or medication hasn’t helped enough, don’t lose hope—there are still other options being explored.
Transcranial magnetic stimulation (TMS)
One emerging treatment is transcranial magnetic stimulation (TMS), a noninvasive therapy that “uses gentle magnetic pulses to calm the part of the brain involved in OCD,” says Dr. Eller. TMS is already FDA-cleared for treatment-resistant OCD in the general population and is typically considered when ERP therapy and medications haven’t provided enough relief.
Research specific to postpartum OCD is still very limited, but early findings are encouraging. In one case report, a form of TMS called theta-burst stimulation appeared to reduce obsessive-compulsive symptoms, at least in the short term.
That said, more studies are needed to understand how safe and effective TMS is for postpartum OCD specifically.
Deep brain stimulation (DBS)
“In the most severe cases, a procedure called Deep Brain Stimulation [DBS] can directly regulate that brain circuit,” says Dr. Eller. This procedure directly targets the brain circuits involved in OCD using implanted electrodes. While the procedure is uncommon and typically a last-resort option, the research is encouraging: studies in the general OCD population show long-term symptom reduction of roughly 47%, with up to 70% of patients experiencing meaningful improvement.
Still, DBS isn’t without risks. Approximately one third of patients experience side effects, though often mild and reversible, and some people report changes in mood, behavior, or sense of self.

Finding the right care for you
If you’re searching for how to stop postpartum intrusive thoughts, finding the right clinician can make all the difference. “If this sounds like you, or someone you love, finding an OCD specialist is an important next step,” says Dr. Eller.
It’s important to work with someone specifically trained in OCD diagnosis and treatment—not just generalized anxiety, which requires a different type of therapy.
When interviewing a provider, ask:
- Are you trained in ERP?
- Do you have experience treating OCD and postpartum OCD specifically?
Two trusted places to start your search:
Both offer provider directories, education, and support resources for postpartum parents navigating OCD and intrusive thoughts.
Relief within reach
Care covered by your insurance
Radial provides advanced mental health treatment, covered by the insurance you already use.








The bottom line
Postpartum OCD can make new parenthood feel terrifying, isolating, and deeply shame-filled, but having intrusive thoughts does not mean you will harm your baby. In fact, people with postpartum OCD are usually distressed precisely because the thoughts feel so out of character and unacceptable to them.
The bright spot: postpartum OCD is treatable. With the right support, many people see major improvement. The hardest part is often speaking up.
If intrusive thoughts, compulsions, or anxiety are taking over your days, Radial can help connect you with licensed clinicians offering fast-acting, evidence-based mental health treatments virtually or in person. Together, you can build a personalized treatment plan designed to help you feel safer, calmer, and more like yourself again.
Key takeaways
- Postpartum OCD causes intrusive, unwanted thoughts and compulsive behaviors centered around the baby, often involving fears of harm, contamination, or mistakes.
- These thoughts are ego-dystonic—they feel horrifying because they go against the parent’s actual values and intentions.
- Postpartum OCD is often mistaken for postpartum anxiety or depression and can be confused with postpartum psychosis—but they are very different conditions.
- Effective treatments exist, including ERP therapy, medication, and emerging options like TMS for treatment-resistant cases.
Frequently asked questions (FAQs)
Is postpartum OCD dangerous?
For the vast majority of people, postpartum OCD does not make them dangerous to their baby. Research shows there’s no link between ego-dystonic intrusive thoughts of infant harm and actually harming an infant.
That said, untreated postpartum OCD can still take a serious toll. Constant fear, compulsive behaviors, and avoidance can interfere with bonding, strain relationships, worsen quality of life, and make daily functioning feel overwhelming. Over time, the stress can affect the well-being of the entire family, which is why getting support and treatment matters.
Can postpartum worsen OCD?
Yes. Research suggests that about 46–50% of people with OCD experience worsening symptoms after childbirth. Likely the same factors linked to postpartum OCD—major hormonal shifts, sleep deprivation, and the intense stress of caring for a newborn—can also intensify preexisting OCD symptoms.
Is it safe to take medication for OCD while breastfeeding?
In many cases, yes. Several medications commonly used for OCD—including the SSRIs fluoxetine, fluvoxamine, paroxetine, and sertraline, as well as the tricyclic antidepressant clomipramine—are generally considered compatible with breastfeeding. While some medication can pass into breast milk, it’s typically in very small amounts.
That said, treatment decisions during breastfeeding are personal. A provider can help you weigh the benefits and risks based on your symptoms, health history, and feeding goals. If you want to research specific medications, trusted resources like the LactMed database (NIH) and MotherToBaby offer evidence-based guidance.
Editorial Standards
At Radial, we believe better health starts with trusted information. Our mission is to empower readers with accurate, accessible, and compassionate content rooted in evidence-based research and reviewed by qualified medical professionals. We’re committed to ensuring the quality and trustworthiness of our content and editorial process–and providing information that is up-to-date, accurate, and relies on evidence-based research and peer-reviewed journals. Learn more about our editorial process.
Let's connect
Get started with finding the right treatment for you or someone you care about
Get startedExplore more posts




