CPTSD vs. BPD: How Complex PTSD and Borderline Personality Disorder Differ

CPTSD and BPD share enough overlapping symptoms that they’re frequently mistaken for one another. Because experts don’t always fully agree on how the conditions are defined, understanding your symptoms and trauma history is often more important than focusing on the diagnosis alone.
Two conditions can share many of the same features on the surface and still be fundamentally different, as is the case with CPTSD vs. BPD.
Complex post-traumatic stress disorder (CPTSD) and borderline personality disorder (BPD) are similar in several ways. "The two conditions share a lot of surface-level features," says Greg Malzberg, MD, a Radial psychiatrist and editor of the Psychofarm Podcast. This includes intense emotional reactions, difficulty in relationships, a troubled sense of self, and often a history of childhood adversity.
Those similarities can sometimes complicate the diagnostic process. "When someone describes all of those things to a clinician, it's genuinely not always obvious which framework fits best, or whether both apply," he says.
Knowing where the two conditions overlap and where they differ can help you better understand your own experiences or those of someone you care about. In this article, we'll take a closer look at each condition, exploring how symptom overlap can sometimes lead to confusion. We'll also cover what clinicians look for during diagnosis and what this might mean for treatment.
What is complex PTSD?
Trauma leaves a lasting mark, including flashbacks, anxiety, and avoiding anything that brings the experience back. But when trauma is repeated, prolonged, and impossible to escape, it can lead to a condition known as complex post-traumatic stress disorder (CPTSD).
The difference between CPTSD and PTSD involves the way trauma occurs. "Complex PTSD is how the mind and body respond to repeated or prolonged traumatic experiences, especially when escape or protection was limited," says MaryEllen Eller, MD, a board-certified psychiatrist and regional medical director at Radial. That's the key distinction from PTSD, which typically follows a single event or discrete events.
Examples include intimate partner violence, ongoing child abuse or neglect, human trafficking, war, political violence, persistent community violence, and ongoing bullying. The “complex” part reflects how ongoing, inescapable trauma shapes a person differently than a one-time crisis.
CPTSD isn’t currently recognized as its own diagnosis in the DSM-5-TR, the handbook most U.S. clinicians use. It tends to be treated as a presentation of PTSD. The World Health Organization’s International Classification of Diseases (ICD-11), however, does list it as a separate condition. That difference can influence how clinicians use these terms.
Healing happens through strong relationships
Compassionate, experienced mental health professionals focused on evidence-based care
%20(1).png)



Core symptoms of CPTSD
According to Dr. Malzberg, CPTSD involves PTSD symptoms like re-experiencing, avoidance, and hyperarousal, plus symptoms related to disturbances in self-organization.
This includes:
- Difficulties regulating emotions
- Negative beliefs about oneself (often involving deep shame)
- Problems maintaining close relationships
"That ‘PTSD plus’ framing is useful, because it means a clinician should be looking for the core trauma symptoms alongside those broader difficulties, not just the broader difficulties alone,” he explains.
What is borderline personality disorder (BPD)?
Those disturbances in self-organization are part of why CPTSD is sometimes confused with borderline personality disorder.
BPD is a type of personality disorder characterized by instability or extreme sensitivity in how people see themselves and the world. Emotions are intense and hard to manage, with frequent mood shifts. It also comes with a deep sensitivity to rejection and a persistent fear of abandonment that often contributes to tumultuous relationships.
What drives it isn’t fully understood, but researchers point to a mix of factors. "Early trauma is a significant risk factor, but it is not the sole cause," Dr. Eller says. Other factors, including neglect, invalidating environments, and unpredictable caregiving, are also believed to play a part. Biological factors, including neurobiological differences and genetics, are also likely involved.
Core symptoms of BPD
- Intense fear of real or perceived abandonment
- Unstable, intense relationships that swing between idealization and devaluation
- Identity disturbances that include an unstable or shifting sense of self
- Impulsivity in at least two areas that are potentially self-damaging (such as reckless behavior, overspending, or substance use)
- Rapidly shifting moods
- Feeling empty
- Intense and inappropriate anger
- Paranoia or dissociation triggered by stress
- Recurrent suicidal behavior, thoughts, or self-harm
Why CPTSD and BPD are often confused
Looking at the similarities, it’s easy to see why CPTSD and BPD can get mixed up. Both involve emotional dysregulation, identity issues, and relationship instability. And while traumatic experiences aren’t required for a BPD diagnosis, an estimated 30% to 90% of people with BPD have a history of childhood abuse and neglect.
Without knowing the full trauma history underneath a patient’s behavior, a clinician might focus on the most visible symptoms, like emotional outbursts or unstable relationships. Because trauma is a particularly sensitive and emotionally fraught area to explore, it is often difficult and takes time to elicit information that could lead to a clear diagnosis. Faced with these factors, subtle but important differences can be missed, and people with complex trauma might end up with a BPD diagnosis, without deeper understanding.
How symptoms present can also play a part in this confusion. Symptoms of BPD are sometimes directed inwardly instead of being expressed outwardly, referred to as quiet BPD. Without some of those visible features that are usually linked to BPD, quiet BPD might be easier to mistake for CPTSD.
Ongoing debate about CPTSD and BPD add to the confusion. "Some see CPTSD as a broader category that BPD can fall within. Others think CPTSD is essentially what happens when you look at the same clinical picture through a trauma-focused lens," says Dr. Malzberg. He notes, "Where one clinician sees BPD, another may genuinely see CPTSD, not because one of them is wrong, but because the categories themselves are still being worked out."

Key differences between CPTSD and BPD
CPTSD and BPD overlap can be confusing on the surface, but research suggests they differ in key areas, particularly in how they affect emotions and behaviors.
Differences in sense of self and identity
Both conditions affect how people see themselves, but in different ways:
- CPTSD: People with CPTSD typically have a persistently negative sense of self. With that negativity comes chronic feelings of guilt, shame, and worthlessness that are rooted in their trauma.
- BPD: In BPD, this issue is less about a negative self-view and more about an unstable one. A person’s identity can shift quickly, leading to sudden changes in self-image, values, goals, and perceptions of their relationships.
Differences in emotional regulation
Both conditions involve difficulty managing emotions, but these patterns look different:
- CPTSD: Emotional reactions are often connected to trauma triggers. When these reminders surface, people feel overwhelmed by intense emotions like anger, sadness, and fear. Others may feel numb or disconnected from their emotions.
- BPD: Emotional responses in BPD are often intense and lead to externalizing behaviors like impulsivity, frantic efforts to prevent abandonment, and outward signs of anger and/or mood reactivity, says Dr. Malzberg.
Differences in relationship patterns and attachment
CPTSD and BPD both make relationships difficult, but these patterns may tend to move in different directions.
- CPTSD: CPTSD often involves a withdrawal response as a way to protect the self from further trauma. People with CPTSD may lean toward avoidant (dismissive) attachment. Trust can feel difficult, and relying on other people often feels unsafe. As a result, they become highly self-reliant and struggle to feel safe and connected in relationships.
- BPD: In contrast, people with BPD crave connection but fear abandonment. This can lead to intense but unstable relationships with a push-pull dynamic. This all-or-nothing type of thinking is known as bpd splitting, and can cause people to idealize their partner one moment and devalue them the next.
Dr. Malzberg emphasizes that these are tendencies, not hard rules. In fact, one can see how these conditions could be two sides of the same coin. Teasing out differences often means looking at whether difficulties followed trauma or reflect longer-standing patterns in how a person sees themselves and others.

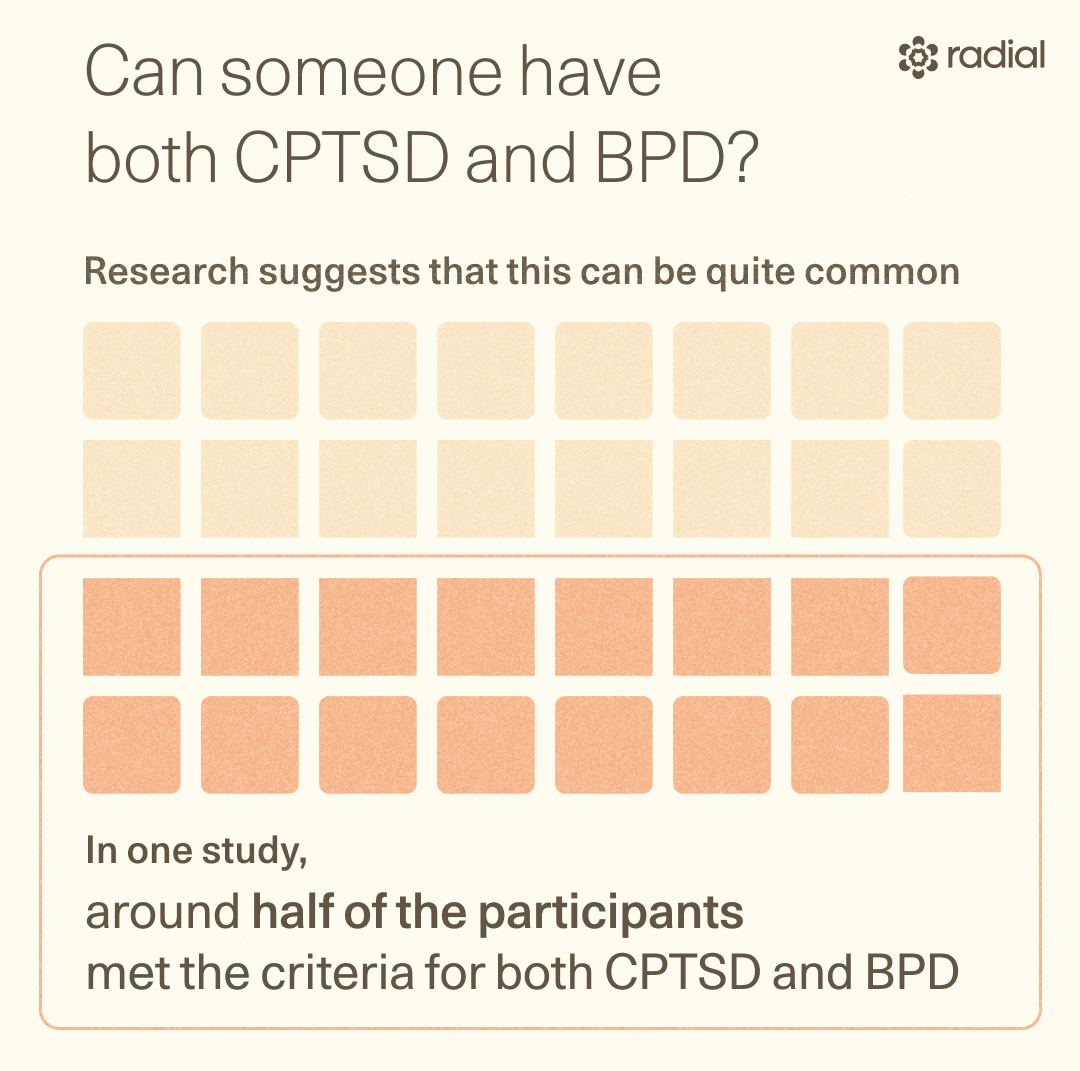
Can someone have both CPTSD and BPD?
People can meet the diagnostic criteria for both complex post-traumatic stress disorder and borderline personality disorder. “Trauma-related symptoms and personality-related patterns can coexist in the same individual,” Dr. Eller explains.
Research suggests that this can be quite common–in one study, around half of the participants met the criteria for CPTSD and BPD. When two conditions occur together, clinicians refer to this as comorbidity.
When someone has symptoms that might be a part of either condition, clinicians will look closely at a person's history, including their experiences with trauma. They may consider whether their emotional responses are primarily linked to reminders of the trauma or whether these reactions reflect more persistent instability in mood, identity, and relationships, which have become generally integrated as traits and ingrained into one’s personality, more reflective of BPD.
"The question isn't always ‘which one is it’ so much as ‘what framework best helps this person understand themselves and get the right treatment,’” Dr. Malzberg explains.
How CPTSD and BPD are treated
Symptoms of CPTSD and BPD can feel distressing and even overwhelming at times, but both are treatable. "Both BPD and CPTSD point toward therapy rather than medication as the primary treatment, and many of the same approaches help with both," Dr. Malzberg says.
CPTSD treatment
The very factors that make CPTSD “complex,” can also make it a bit more challenging to treat. The condition takes time to develop, so treatments need to address deeply rooted emotional and behavioral patterns.
"Therapy is a powerful tool for re-establishing trust and adjusting the way we relate to other people," Dr. Eller explains. "Therapy also helps us adjust the narrative or lies that trauma led us to believe and evaluate the world in more accurate, helpful ways."
Some of these options include:
- Trauma-focused CBT: This form of cognitive-behavioral therapy focuses on identifying and changing distorted thinking patterns and stress responses, helping people better manage symptoms.
- EMDR: Eye movement and desensitization and reprocessing therapy uses guided eye movements to help process traumatic memories and emotions. This can make memories of those experiences less overwhelming over time.
- Cognitive processing therapy: A form of CBT that challenges people to change their distortions so they can better learn to trust and value their own worth.
- Neurotherapy: Dr. Eller points to Prism Neurofeedback, which tracks brainwaves to help the nervous system learn to calm its threat response, and Transcranial Magnetic Stimulation (TMS), which is showing early results for improving mood regulation, anxiety, and sleep in people with PTSD.
- Psychedelic therapy: Psychedelic-assisted therapy is also an active area of research, with early studies on psilocybin-based treatment and MDMA producing promising early signals, Dr. Eller says. (Disclaimer: MDMA-assisted therapy is still experimental, and experts have raised concerns about study design. There are still questions about how safety issues and study data were reported. More rigorous research is still needed.)
- Medications: While therapy is the primary treatment for CPTSD, medications can sometimes help people manage symptoms like anxiety, insomnia, or depression. Antidepressants, anti-anxiety medications, and mood stabilizers can make it easier to function in daily life and support therapy. A medication prazosin is often helpful in reducing PTSD-related nightmares.
Dr. Eller notes that while SSRIs can reduce symptom intensity for some people, results are mixed, and benzodiazepines, once commonly used for severe anxiety, are no longer recommended for PTSD as some research suggests they can worsen symptoms over time.
Relief within reach
Care covered by your insurance
Radial provides advanced mental health treatment, covered by the insurance you already use.








BPD treatment
Borderline personality disorder is also treatable with the right therapy and support. Like CPTSD, treatments typically focus on therapy, but medications may sometimes help with specific symptoms.
- Dialectical behavior therapy (DBT): DBT was specifically developed for the treatment of BPD. It teaches people skills to help them manage emotions, improve relationships, tolerate distress, and stay mindful of their feelings.
- Mentalization-based therapy (MBT): MBT helps people understand their own thoughts and emotions as well as those of others. People respond less impulsively and build healthier connections with others, leading to meaningful reductions in BPD symptoms, including fewer interpersonal issues and less emotional distress.
- Transference-focused psychotherapy (TFP): TFP is a structured psychodynamic treatment that helps people develop a stable sense of self and improve relationships through the therapeutic relationship. Research suggests it can reduce BPD symptoms and improve functioning.
- Schema therapy: This approach helps people recognize and change long-standing patterns (aka “schemas”) that contribute to unhelpful behaviors and emotional distress. By challenging negative beliefs about themselves and their relationships with others, people can improve their functioning and reduce overall BPD symptoms.
- Medications: There are no medications that specifically treat BPD, but medication can help ease symptoms like mood swings, depression, and anxiety. Medications are usually used alongside therapy rather than on their own to improve daily functioning while people work on long-term coping strategies.
When to seek professional support
Healing from trauma, learning to navigate intense emotions, and building stronger relationships all take strength. Asking for help can put you on the path to feeling more stable and supported.
It may be time to seek professional help if you notice:
- Frequent mood swings and emotional outbursts
- Intrusive memories, anxiety, or reminders of past trauma
- Intense emotions that are hard to manage
- Persistent feelings of shame, worthlessness, or emptiness
- Difficulty trusting others or maintaining stable relationships
- Self-harm, suicidal thoughts, or risky behaviors
If these symptoms and patterns are affecting your daily life, including your work and relationships, it's important to talk to a mental health professional. Starting the conversation can be tough, but it can be as simple as telling your doctor or therapist about some of the symptoms you've been having.
And if you think your current diagnosis doesn’t fully capture your experiences, talk to your clinician. "The most important question isn't really which label you have. It's whether your clinician's understanding of you actually fits your experience, and whether the treatment you're being offered makes sense given what you're going through," says Dr. Malzberg.
The bottom line
If you're trying to make sense of symptoms you've been experiencing, the key thing to remember is that both CPTSD and BPD are treatable. Getting the right diagnosis is the first step toward making sense of your symptoms and finding the right care.
Understanding your experiences can be easier with the right kind of support. Connect with a Radial clinician experienced in trauma and personality disorders to explore your symptoms and find a treatment approach that works for you.
Key takeaways
- CPTSD and BPD haveshare some overlapping symptoms, but also differ in how they affect the sense of self, emotional regulation, and relationship patterns.
- While CPTSD stems from prolonged, inescapable trauma, BPD has many contributing factors and can develop without a history of trauma.
- The overlap between the conditions can lead to confusion and misdiagnosis, so talking to an experienced clinician is key.
- While distressing, both conditions are treatable with therapy, including trauma-focused approaches, cognitive treatments, and newer options like neurotherapy.
Frequently asked questions
How do you know if you have CPTSD or BPD?
The overlap between the two makes it hard to decipher on your own which condition it might be. This is exactly why getting a professional evaluation matters. A qualified mental health clinician can assess your symptoms and history to figure out if what you are experiencing is better explained by CPTSD, BPD, or something else altogether.
That said, there are some patterns you can note on your own. Symptoms that begin or worsen after prolonged trauma, combined with a persistently negative sense of self, point more toward CPTSD. Rapid mood shifts, intense fear of abandonment, and turbulent relationships are more characteristic of BPD. But these are signs, not a diagnosis, which only a clinician can give.
What can CPTSD be mistaken for?
CPTSD can be misdiagnosed as anxiety,PTSD, BPD, bipolar disorder, or depression. All of these conditions involve emotional dysregulation, negative self-perception, and relationship difficulties. Part of the challenge is that CPTSD is still relatively new as a diagnosis in the ICD-11 and isn't used in all clinical settings. What often separates CPTSD from these other conditions is the overall picture, which involves a history of repeated trauma alongside feelings of guilt and shame that are clearly rooted in those early experiences.
Can trauma cause BPD?
Trauma, particularly in early childhood, can play a role in BPD, but it’s neither the only factor nor a requirement for diagnosis. Experiences like neglect, abuse, and inconsistent caregiving interact with neurological differences and genetics to raise a person's risk. The result is that BPD emerges from a combination of biological, psychological, and environmental factors rather than trauma alone.
What should I do if I think I was misdiagnosed?
If something doesn't feel right about your diagnosis or recommended treatment, it's okay to ask your provider questions or even seek a second opinion.
"If you suspect a misdiagnosis, the most important question isn't really which label you have. It's whether your clinician's understanding of you actually fits your experience, and whether the treatment you're being offered makes sense given what you're going through," Dr. Malzberg says.
Start by talking about your concerns with a mental health professional and giving them as much context as you can, including details about your symptoms, history, and anything about how your current treatment doesn’t seem to be helping. “A good clinician will welcome a direct conversation about their thinking, and that conversation is worth having,” Dr. Malzberg notes. This conversation can clarify what's going on, give you greater peace of mind, and ensure you're getting the right kind of support.
Deep dive recommendations
- Psychiatry & Psychotherapy Podcast. Episode 215: Understanding complex PTSD and borderline personality disorder.
- Psychofarm. CPTSD vs. BPD: How to think about the difference and what to do about it.
Editorial Standards
At Radial, we believe better health starts with trusted information. Our mission is to empower readers with accurate, accessible, and compassionate content rooted in evidence-based research and reviewed by qualified medical professionals. We’re committed to ensuring the quality and trustworthiness of our content and editorial process–and providing information that is up-to-date, accurate, and relies on evidence-based research and peer-reviewed journals. Learn more about our editorial process.
Let's connect
Get started with finding the right treatment for you or someone you care about
Get startedExplore more posts